

Real-World Effectiveness of Intravenous and Oral Antibiotic Stepdown Strategies for Gram-Negative Complicated Urinary Tract Infection With Bacteremia
- PMID: 38665174
- PMCID: PMC11045028
- DOI: 10.1093/ofid/ofae193
Real-World Effectiveness of Intravenous and Oral Antibiotic Stepdown Strategies for Gram-Negative Complicated Urinary Tract Infection With Bacteremia
Abstract
Background: Robust data are lacking regarding the optimal route, duration, and antibiotic choice for gram-negative bloodstream infection from a complicated urinary tract infection source (GN-BSI/cUTI).
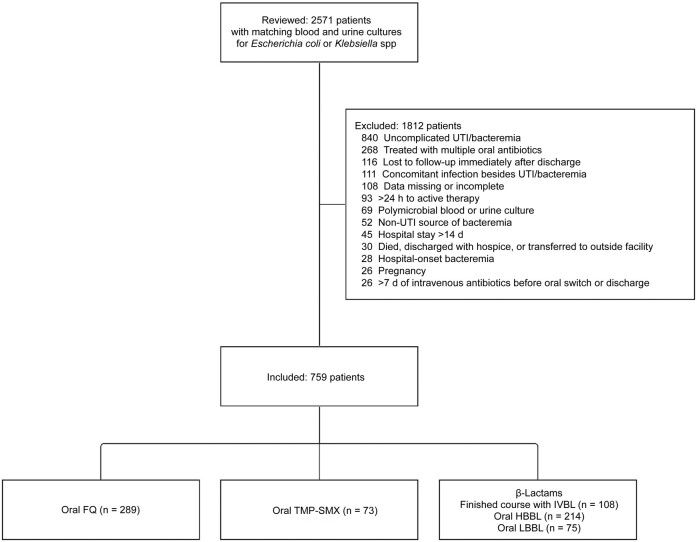
Methods: In this multicenter observational cohort study, we simulated a 4-arm registry trial using a causal inference method to compare effectiveness of the following regimens for GN-BSI/cUTI: complete course of an intravenous β-lactam (IVBL) or oral stepdown therapy within 7 days using fluoroquinolones (FQs), trimethoprim-sulfamethoxazole (TMP-SMX), or high-bioavailability β-lactams (HBBLs). Adults treated between January 2016 and December 2022 for Escherichia coli or Klebsiella species GN-BSI/cUTI were included. Propensity weighting was used to balance characteristics between groups. The 60-day recurrence was compared using a multinomial Cox proportional hazards model with probability of treatment weighting.
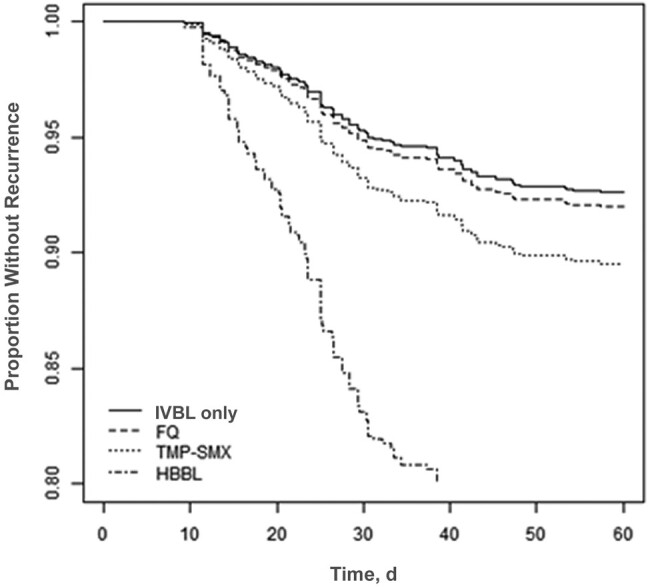
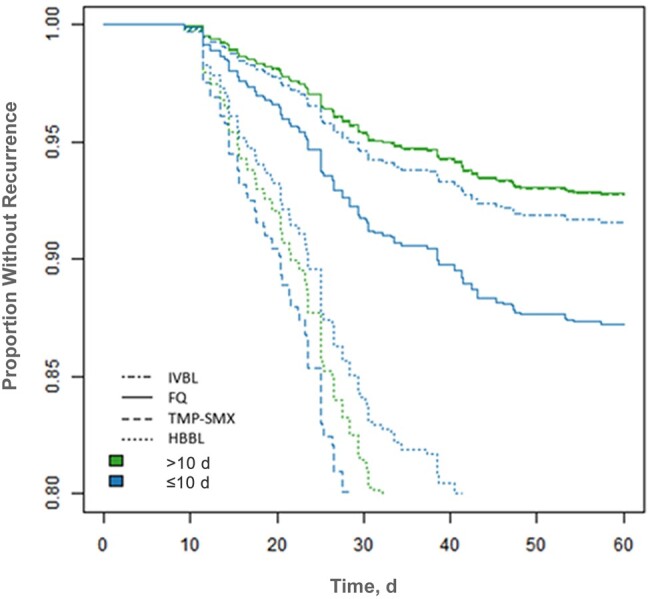
Results: Of 2571 patients screened, 759 (30%) were included. Characteristics were similar between groups. Compared with IVBLs, we did not observe a difference in effectiveness for FQs (adjusted hazard ratio, 1.09 [95% confidence interval, .49-2.43]) or TMP-SMX (1.44 [.54-3.87]), and the effectiveness of TMP-SMX/FQ appeared to be optimal at durations of >10 days. HBBLs were associated with nearly 4-fold higher risk of recurrence (adjusted hazard ratio, 3.83 [95% confidence interval, 1.76-8.33]), which was not mitigated by longer treatment durations. Most HBBLs (67%) were not optimally dosed for bacteremia. Results were robust to multiple sensitivity analyses.
Conclusions: These real-world data suggest that oral stepdown therapy with FQs or TMP-SMX have similar effectiveness as IVBLs. HBBLs were associated with higher recurrence rates, but dosing was suboptimal. Further data are needed to define optimal dosing and duration to mitigate treatment failures.
Keywords: antimicrobial stewardship; complicated urinary tract infection; gram-negative bacteremia; real-world evidence; β-lactams.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts of interest.
Figures
References
-
- Tamma PD, Cosgrove SE. Which trial do we need? Early oral antibiotic therapy for the treatment of gram-negative bloodstream infections. Clin Microbiol Infect 2023; 29:670–2. - PubMed
-
- Omrani AS, Abujarir SH, Ben Abid F, et al. Switch to oral antibiotics in gram-negative bacteraemia: a randomized, open-label, clinical trial. Clin Microbiol Infect 2024; 30:492–498. - PubMed
