

A comparative study to evaluate the cervical spine movements during laryngoscopy using Macintosh and Airtraq laryngoscopes
- PMID: 38666159
- PMCID: PMC11042109
- DOI: 10.4103/joacp.joacp_89_22
A comparative study to evaluate the cervical spine movements during laryngoscopy using Macintosh and Airtraq laryngoscopes
Abstract
Background and aim: Intubation with Macintosh requires flexing the lower cervical spine and extending the atlanto-occipital joint to create a "line of sight." Primary aim of study was to compare the extent of cervical spine movement during laryngoscopy using conventional Macintosh laryngoscope and Airtraq.
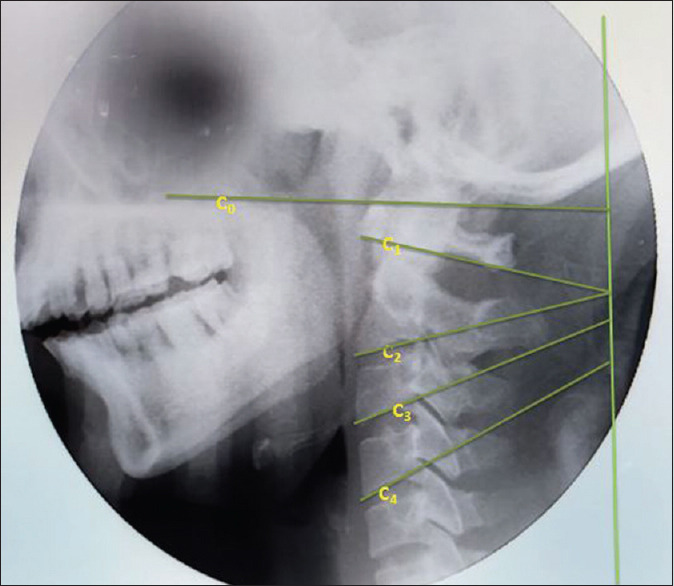
Material and methods: A total of 25 patients of either sex between the age group of 18 and 60 years, having American Society of Anesthesiologists (ASA) physical status of Grade-I and Grade-II, scheduled for elective surgery under image control requiring general anesthesia and intubation were enrolled. A baseline image of the lateral cervical spine including the first four cervical vertebrae was taken by an image intensifier. After administration of general anesthesia, laryngoscopy was first performed using a Macintosh laryngoscope and a second X-ray image of the lateral cervical spine was taken. The second laryngoscopy using a Airtraq laryngoscope was done and the third image of the lateral cervical spine was taken. Angles between occiput and C1; C1 and C2; C2 and C3; C3 and C4; and occiput and C4 were calculated. Atlanto-occipital distance (AOD) was calculated as the distance between occiput and C1.
Results: Macintosh showed greater cervical movement as compared with Airtraq but a significant difference in the movement was observed at C2-C3 and C0-C4. Baseline mean AOD was 2.21 ± 1.25 mm, after Macintosh and Airtraq laryngoscopy was found to be 1.13 ± 0.60 and 1.6 ± 0.78 mm, respectively, and was found to be significant (P < 0.05).
Conclusion: We conclude that Airtraq allows intubation with less movement of the upper cervical spine makes Airtraq preferred equipment for intubation in patients with a potential cervical spine injury.
Keywords: Cervical vertebrae; general anesthesia; intubation; laryngoscope; laryngoscopy; spine.
Copyright: © 2023 Journal of Anaesthesiology Clinical Pharmacology.
Conflict of interest statement
There are no conflicts of interest.
Figures





References
-
- Sawin PD, Todd MM, Traynelis VC, Farrell SB, Nader A, Sato Y, et al. Cervical spine motion with direct laryngoscopy and orotracheal intubation: An in vivo cinefluoroscopic study of subjects without cervical abnormality. J Am Soc Anesthesiol. 1996;85:26–36. - PubMed
-
- Takenaka I, Aoyama K, Iwagaki T, Ishimura H, Kadoya T. The sniffing position provides greater occipitoatlanto-axial angulation than simple head extension: A radiological study. Can J Anesth. 2007;54:129–33. - PubMed
-
- Saracoglu KT, Eti Z, Gogus FY. Airtraq optical laryngoscope: Advantages and disadvantages. Middle East J Anaesthesiol. 2013;22:135–41. - PubMed
-
- Hirabayashi Y, Fujita A, Seo N, Sugimoto H. A comparison of cervical spine movement during laryngoscopy using the Airtraq®or Macintosh laryngoscopes. Anaesthesia. 2008;63:635–40. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous