

Rebound Inverts the Staphylococcus aureus Bacteremia Prevention Effect of Antibiotic Based Decontamination Interventions in ICU Cohorts with Prolonged Length of Stay
- PMID: 38666992
- PMCID: PMC11047347
- DOI: 10.3390/antibiotics13040316
Rebound Inverts the Staphylococcus aureus Bacteremia Prevention Effect of Antibiotic Based Decontamination Interventions in ICU Cohorts with Prolonged Length of Stay
Abstract
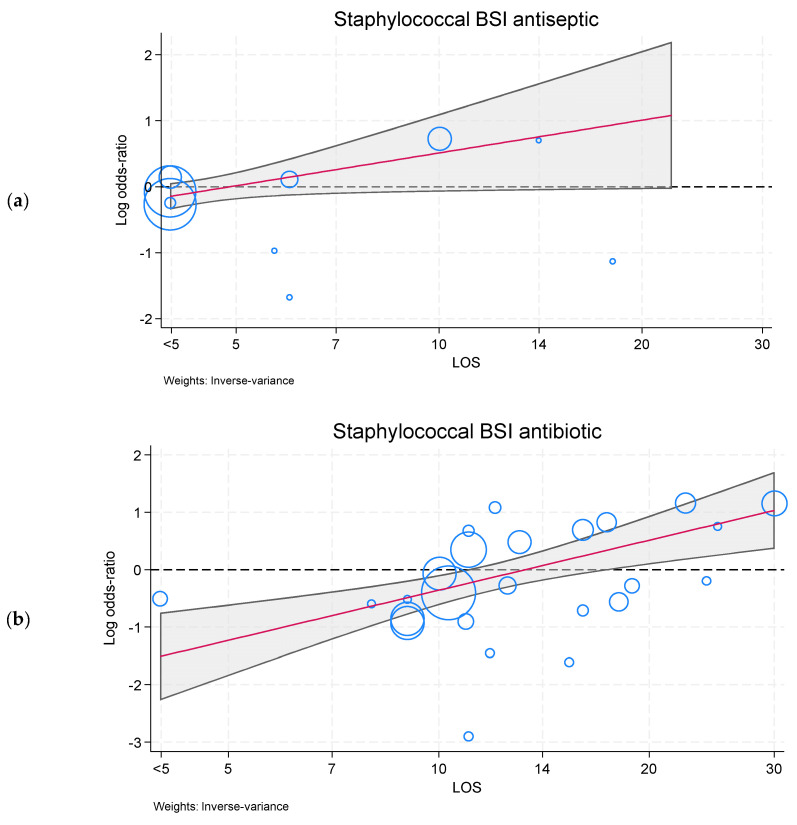
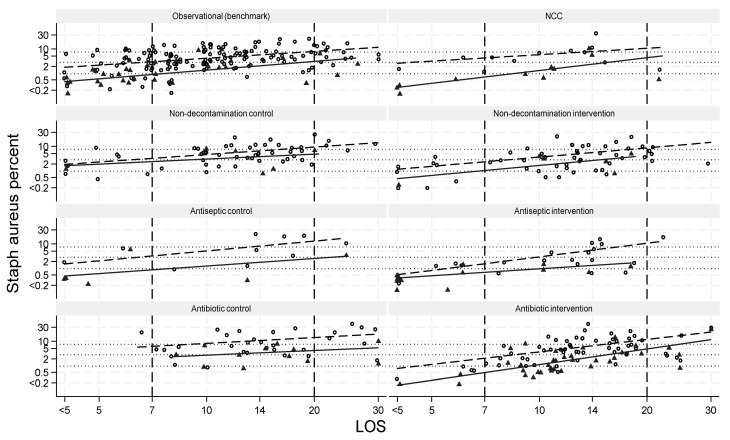
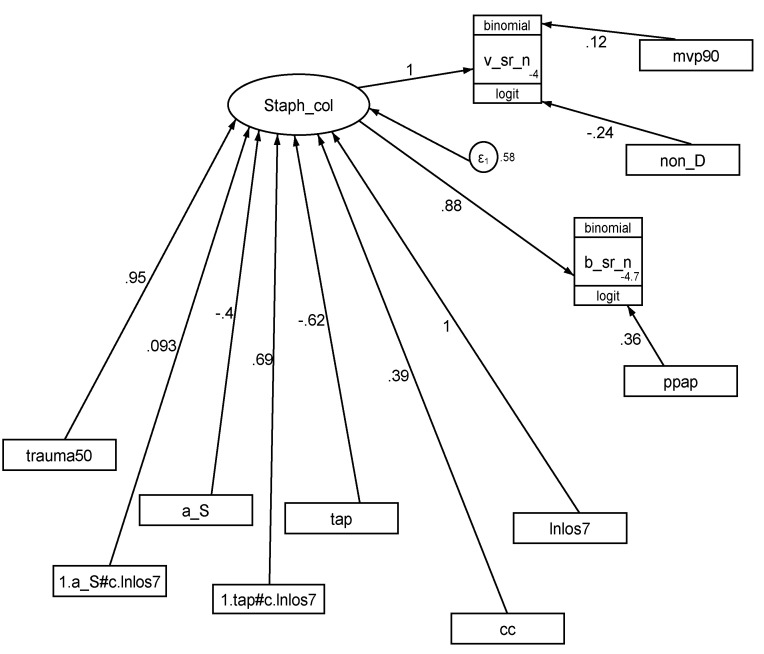
Could rebound explain the paradoxical lack of prevention effect against Staphylococcus aureus blood stream infections (BSIs) with antibiotic-based decontamination intervention (BDI) methods among studies of ICU patients within the literature? Two meta-regression models were applied, each versus the group mean length of stay (LOS). Firstly, the prevention effects against S. aureus BSI [and S. aureus VAP] among 136 studies of antibiotic-BDI versus other interventions were analyzed. Secondly, the S. aureus BSI [and S. aureus VAP] incidence in 268 control and intervention cohorts from studies of antibiotic-BDI versus that among 165 observational cohorts as a benchmark was modelled. In model one, the meta-regression line versus group mean LOS crossed the null, with the antibiotic-BDI prevention effect against S. aureus BSI at mean LOS day 7 (OR 0.45; 0.30 to 0.68) inverted at mean LOS day 20 (OR 1.7; 1.1 to 2.6). In model two, the meta-regression line versus group mean LOS crossed the benchmark line, and the predicted S. aureus BSI incidence for antibiotic-BDI groups was 0.47; 0.09-0.84 percentage points below versus 3.0; 0.12-5.9 above the benchmark in studies with 7 versus 20 days mean LOS, respectively. Rebound within the intervention groups attenuated and inverted the prevention effect of antibiotic-BDI against S. aureus VAP and BSI, respectively. This explains the paradoxical findings.
Keywords: Staphylococcus aureus; antibiotic-based decontamination; bacteremia; intensive care unit; meta-regression; rebound; selective digestive decontamination; spill-over; structural equation model.
Conflict of interest statement
The author declares no conflicts of interest.
Figures
Similar articles
-
Estimating the herd effects of anti-microbial-based decontamination (ABD) interventions on intensive care unit (ICU) acquired bloodstream infections: a deductive meta-analysis.BMJ Open. 2024 Nov 20;14(11):e092030. doi: 10.1136/bmjopen-2024-092030. BMJ Open. 2024. PMID: 39572099 Free PMC article.
-
Unusually High Incidences of Staphylococcus aureus Infection within Studies of Ventilator Associated Pneumonia Prevention Using Topical Antibiotics: Benchmarking the Evidence Base.Microorganisms. 2018 Jan 4;6(1):2. doi: 10.3390/microorganisms6010002. Microorganisms. 2018. PMID: 29300363 Free PMC article.
-
Length of intensive care unit stay and the apparent efficacy of antimicrobial-based versus non-antimicrobial-based ventilator pneumonia prevention interventions within the Cochrane review database.J Hosp Infect. 2023 Oct;140:46-53. doi: 10.1016/j.jhin.2023.07.018. Epub 2023 Aug 4. J Hosp Infect. 2023. PMID: 37544366
-
Topical antibiotics as a major contextual hazard toward bacteremia within selective digestive decontamination studies: a meta-analysis.BMC Infect Dis. 2014 Dec 31;14:714. doi: 10.1186/s12879-014-0714-x. BMC Infect Dis. 2014. PMID: 25551776 Free PMC article. Review.
-
Structural equation modeling the "control of gut overgrowth" in the prevention of ICU-acquired Gram-negative infection.Crit Care. 2020 May 4;24(1):189. doi: 10.1186/s13054-020-02906-6. Crit Care. 2020. PMID: 32366267 Free PMC article.
Cited by
-
Visualizing and diagnosing spillover within randomized concurrent controlled trials through the application of diagnostic test assessment methods.BMC Med Res Methodol. 2024 Aug 16;24(1):182. doi: 10.1186/s12874-024-02296-1. BMC Med Res Methodol. 2024. PMID: 39152400 Free PMC article.
References
-
- Paling F.P., Hazard D., Bonten M.J., Goossens H., Jafri H.S., Malhotra-Kumar S., Sifakis F., Weber S., Kluytmans J.A., ASPIRE-ICU Study Team Association of Staphylococcus aureus colonization and pneumonia in the intensive care unit. JAMA Netw. Open. 2020;3:e2012741. doi: 10.1001/jamanetworkopen.2020.12741. - DOI - PMC - PubMed
-
- Paling F.P., Wolkewitz M., Bode L.G., Klouwenberg P.K., Ong D.S., Depuydt P., de Bus L., Sifakis F., Bonten M.J., Kluytmans J.A. Staphylococcus aureus colonization at ICU admission as a risk factor for developing S. aureus ICU pneumonia. Clin. Microbiol. Infect. 2017;23:49.e9–49.e14. doi: 10.1016/j.cmi.2016.09.022. - DOI - PubMed
-
- Masse J., Elkalioubie A., Blazejewski C., Ledoux G., Wallet F., Poissy J., Preau S., Nseir S. Colonization pressure as a risk factor of ICU-acquired multidrug resistant bacteria: A prospective observational study. Eur. J. Clin. Microbiol. Infect. Dis. 2017;36:797–805. doi: 10.1007/s10096-016-2863-x. - DOI - PubMed
-
- Masse J., Elkalioubie A., Blazejewski C., Ledoux G., Wallet F., Poissy J., Preau S., Nseir S. “Colonization pressure” and risk of acquisition of methicillin-resistant Staphylococcus aureus in a medical intensive care unit. Infect. Control Hosp. Epidemiol. 2000;21:718–723. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
