

High Level of CD8+PD-1+ Cells in Patients with Chronic Myeloid Leukemia Who Experienced Loss of MMR after Imatinib Discontinuation
- PMID: 38667336
- PMCID: PMC11048908
- DOI: 10.3390/cells13080723
High Level of CD8+PD-1+ Cells in Patients with Chronic Myeloid Leukemia Who Experienced Loss of MMR after Imatinib Discontinuation
Abstract
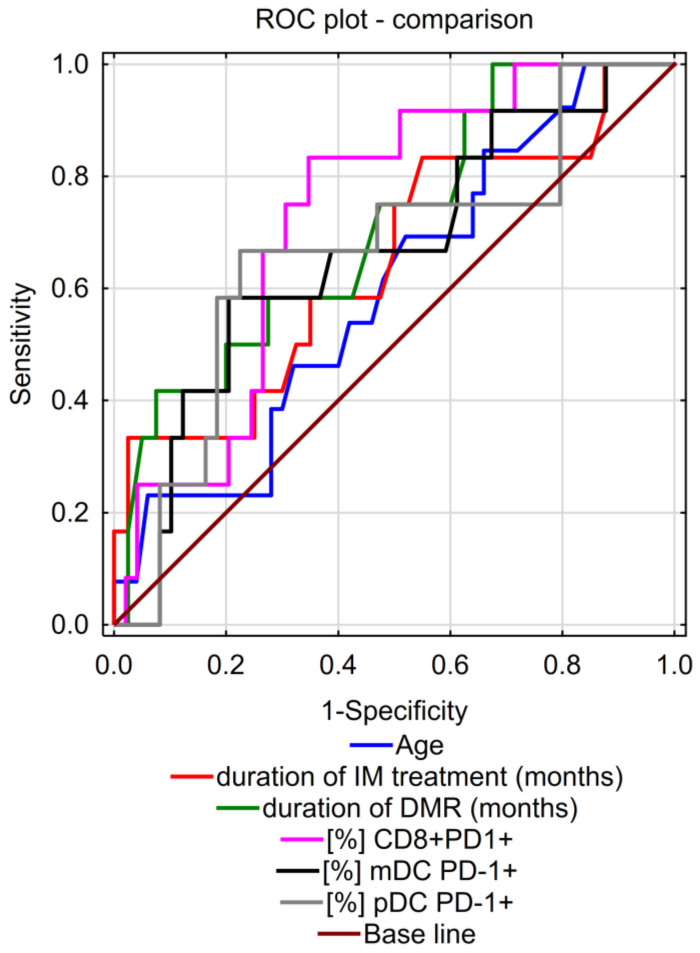
Treatment-free remission (TFR) is achieved in approximately half of chronic myeloid leukemia (CML) patients treated with tyrosine kinase inhibitors. The mechanisms responsible for TFR maintenance remain elusive. This study aimed to identify immune markers responsible for the control of residual CML cells early in the TFR (at 3 months), which may be the key to achieving long-term TFR and relapse-free survival (RFS) after discontinuation of imatinib. Our study included 63 CML patients after imatinib discontinuation, in whom comprehensive analysis of changes in the immune system was performed by flow cytometry, and changes in the BCR::ABL1 transcript levels were assessed by RQ-PCR and ddPCR. We demonstrated a significant increase in the percentage of CD8+PD-1+ cells in patients losing TFR. The level of CD8+PD-1+ cells is inversely related to the duration of treatment and incidence of deep molecular response (DMR) before discontinuation. Analysis of the ROC curve showed that the percentage of CD8+PD-1+ cells may be a significant factor in early molecular recurrence. Interestingly, at 3 months of TFR, patients with the e13a2 transcript had a significantly higher proportion of the PD-1-expressing immune cells compared to patients with the e14a2. Our results suggest the important involvement of CD8+PD-1+ cells in the success of TFR and may help in identifying a group of patients who could successfully discontinue imatinib.
Keywords: chronic myeloid leukemia (CML); discontinuation of imatinib; immune biomarker; treatment-free remission (TFR).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Islamagic E., Hasic A., Kurtovic S., Suljovic Hadzimesic E., Mehinovic L., Kozaric M., Kurtovic-Kozaric A. The Efficacy of Generic Imatinib as First- and Second-Line Therapy: 3-Year Follow-up of Patients With Chronic Myeloid Leukemia. Clin. Lymphoma Myeloma Leuk. 2017;17:238–240. doi: 10.1016/j.clml.2017.02.001. - DOI - PubMed
-
- Hochhaus A., Baccarani M., Silver R.T., Schiffer C., Apperley J.F., Cervantes F., Clark R.E., Cortes J.E., Deininger M.W., Guilhot F., et al. European LeukemiaNet 2020 Recommendations for Treating Chronic Myeloid Leukemia. Leukemia. 2020;34:966–984. doi: 10.1038/s41375-020-0776-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
