

Thalamo-mesencephalic Branches of the Posterior Cerebral Artery: a 3D Rotational Angiography Study
- PMID: 38668868
- PMCID: PMC11339114
- DOI: 10.1007/s00062-024-01418-y
Thalamo-mesencephalic Branches of the Posterior Cerebral Artery: a 3D Rotational Angiography Study
Abstract
Purpose: The thalamo-mesencephalic (TM) branches of the posterior cerebral artery (PCA) supply critical structures. Previous descriptions of these vessels are inconsistent and almost exclusively rely on cadaver studies. We aimed to provide a neuroradiological description of TM vessels in vivo based on routine 3D rotational angiographies (3D-RA).
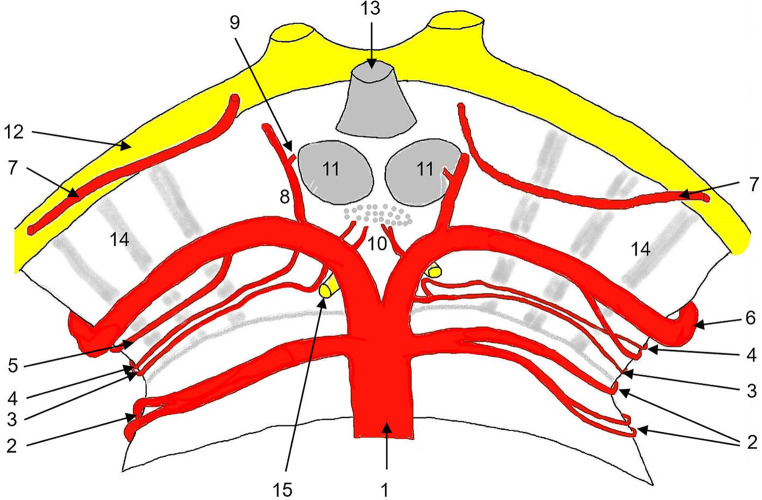
Methods: We analyzed 3D-RAs of 58 patients with pathologies remote from the PCA. PCA-origins were considered. Delineation, origin and number of branches of the collicular artery (CA), the accessory CA (ACA), the posterior thalamoperforating artery (PTA), the thalamogeniculate artery (TGA), and the posterior medial (PMCA) and lateral (PCLA) choroid arteries were assessed. The PTAs were categorized based on Percheron's suggested classification.
Results: A CA was identified in 84%, an ACA in 20%. The PTA was delineated in 100%. In 27%, PTA anatomy had features of several Percheron types (n = 7) or vessels emanating from a net like origin (n = 9). 26% had a type IIb PTA. A fetal type PCA origin with hypoplastic ipsilateral P1 was observed in 5 cases with type IIa (n = 2) or type IIb (n = 3) PTAs originating from contralateral P1. The TGA was identified in 85% of patients, with ≥ 2 branches in 67%. The PMCA was delineable in 41%, the PLCA in 100%.
Conclusion: The prevalence of a proper "Artery of Percheron" type IIb PTA seems to be higher than previously reported. A fetal type P1-origin may be predictive of a type IIa/b PTA emanating from contralateral P1. 3D-RA may be useful for planning PCA interventions, as impairment of TM branches is a severe risk.
Keywords: Digital subtraction angiography; Mesencephalon; Neuroanatomy; Posterior cerebral artery; Thalamus.
© 2024. The Author(s).
Conflict of interest statement
M. Rauch, J. Berkefeld, M. Klonowski, E. Hattingen and S. Weidauer declare that they have no competing interests.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
