

Subcutaneous Administration of a Monoclonal Antibody to Prevent Malaria
- PMID: 38669354
- PMCID: PMC11238904
- DOI: 10.1056/NEJMoa2312775
Subcutaneous Administration of a Monoclonal Antibody to Prevent Malaria
Abstract
Background: Subcutaneous administration of the monoclonal antibody L9LS protected adults against controlled Plasmodium falciparum infection in a phase 1 trial. Whether a monoclonal antibody administered subcutaneously can protect children from P. falciparum infection in a region where this organism is endemic is unclear.
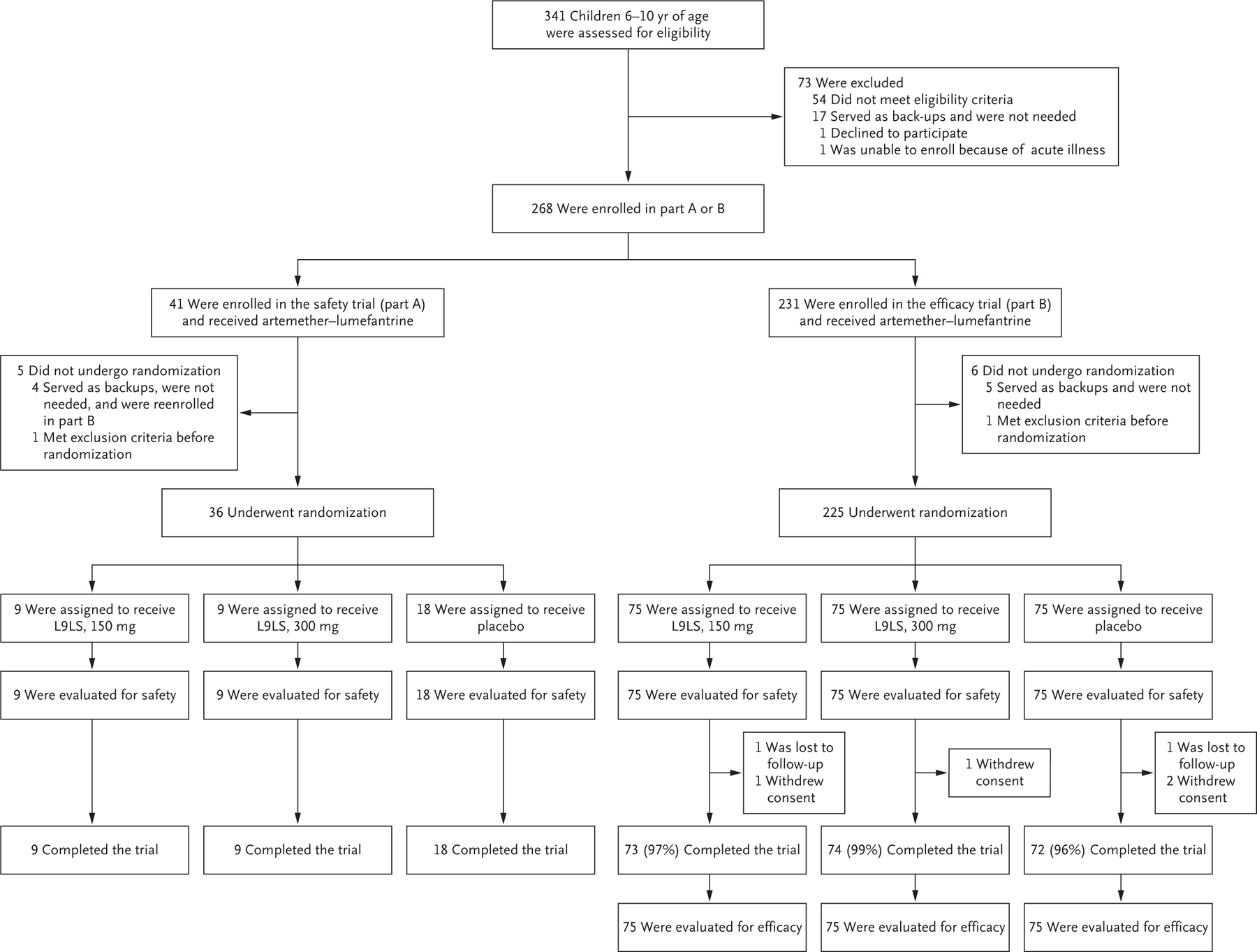
Methods: We conducted a phase 2 trial in Mali to assess the safety and efficacy of subcutaneous administration of L9LS in children 6 to 10 years of age over a 6-month malaria season. In part A of the trial, safety was assessed at three dose levels in adults, followed by assessment at two dose levels in children. In part B of the trial, children were randomly assigned, in a 1:1:1 ratio, to receive 150 mg of L9LS, 300 mg of L9LS, or placebo. The primary efficacy end point, assessed in a time-to-event analysis, was the first P. falciparum infection, as detected on blood smear performed at least every 2 weeks for 24 weeks. A secondary efficacy end point was the first episode of clinical malaria, as assessed in a time-to-event analysis.
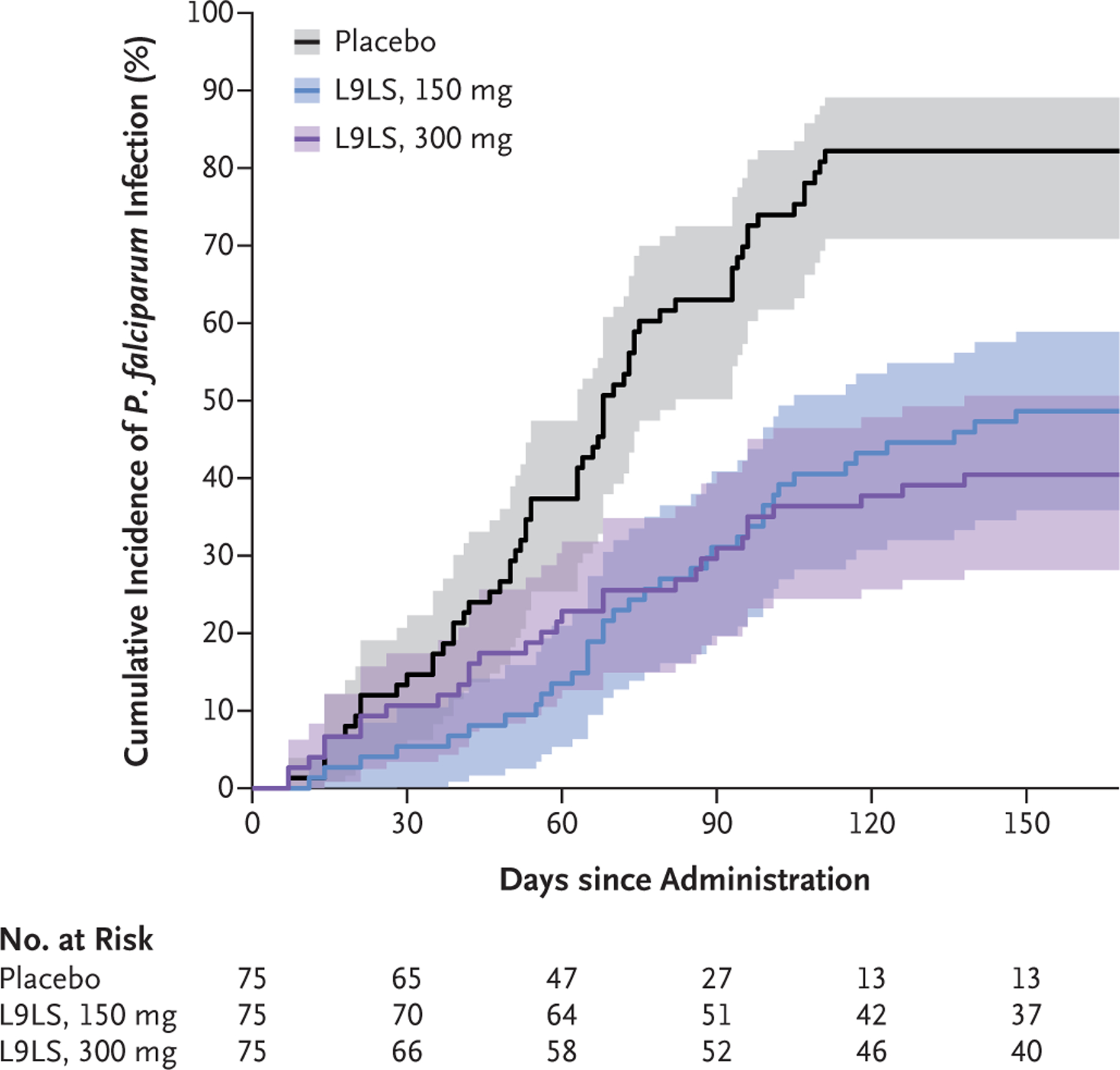
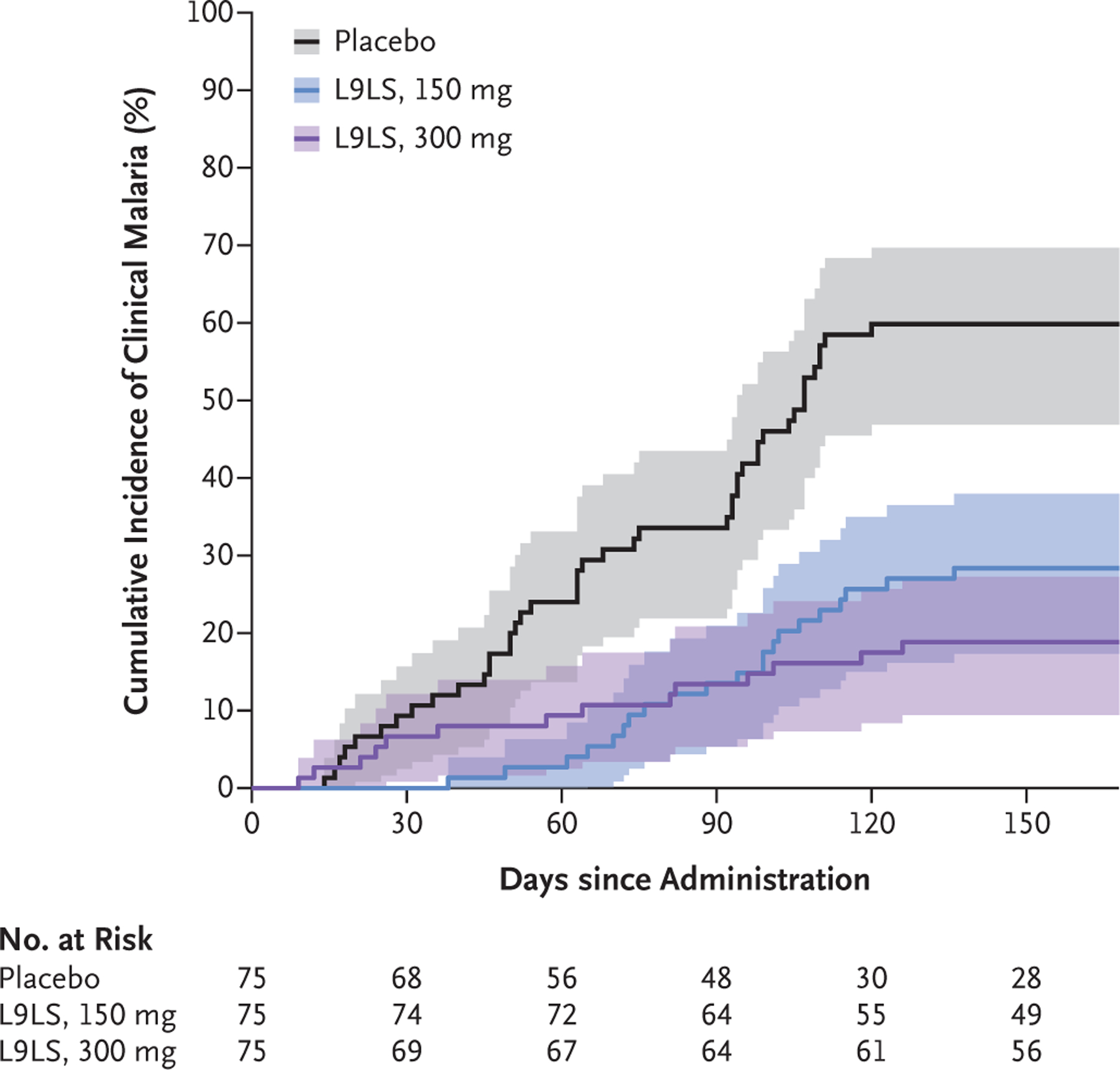
Results: No safety concerns were identified in the dose-escalation part of the trial (part A). In part B, 225 children underwent randomization, with 75 children assigned to each group. No safety concerns were identified in part B. P. falciparum infection occurred in 36 participants (48%) in the 150-mg group, in 30 (40%) in the 300-mg group, and in 61 (81%) in the placebo group. The efficacy of L9LS against P. falciparum infection, as compared with placebo, was 66% (adjusted confidence interval [95% CI], 45 to 79) with the 150-mg dose and 70% (adjusted 95% CI, 50 to 82) with the 300-mg dose (P<0.001 for both comparisons). Efficacy against clinical malaria was 67% (adjusted 95% CI, 39 to 82) with the 150-mg dose and 77% (adjusted 95% CI, 55 to 89) with the 300-mg dose (P<0.001 for both comparisons).
Conclusions: Subcutaneous administration of L9LS to children was protective against P. falciparum infection and clinical malaria over a period of 6 months. (Funded by the National Institute of Allergy and Infectious Diseases; ClinicalTrials.gov number, NCT05304611.).
Copyright © 2024 Massachusetts Medical Society.
Figures
References
-
- World Health Organization. World malaria report 2023 (https://www.who.int/teams/global-malaria-programme/reports/world-malaria...).
-
- Malaria vaccine: WHO position paper — March 2022. Wkly Epidemiol Rec 2022;97: 61–80 (https://iris.who.int/bitstream/handle/10665/352332/WER9709-eng-fre.pdf).
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical