

Predictors of Loss of Ambulation in Duchenne Muscular Dystrophy: A Systematic Review and Meta-Analysis
- PMID: 38669554
- PMCID: PMC11091649
- DOI: 10.3233/JND-230220
Predictors of Loss of Ambulation in Duchenne Muscular Dystrophy: A Systematic Review and Meta-Analysis
Erratum in
-
Corrigendum to "Predictors of Loss of Ambulation in Duchenne Muscular Dystrophy: A Systematic Review and Meta-Analysis".J Neuromuscul Dis. 2025 Jan-Feb;12(1):22143602251320076. doi: 10.1177/22143602251320076. J Neuromuscul Dis. 2025. PMID: 40012473 No abstract available.
Abstract
Objective: The objective of this study was to describe predictors of loss of ambulation in Duchenne muscular dystrophy (DMD).
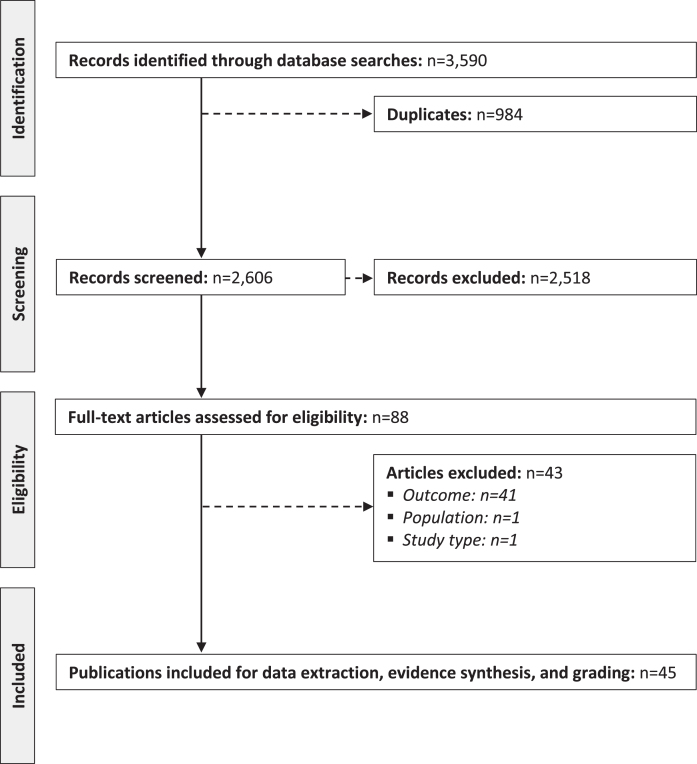
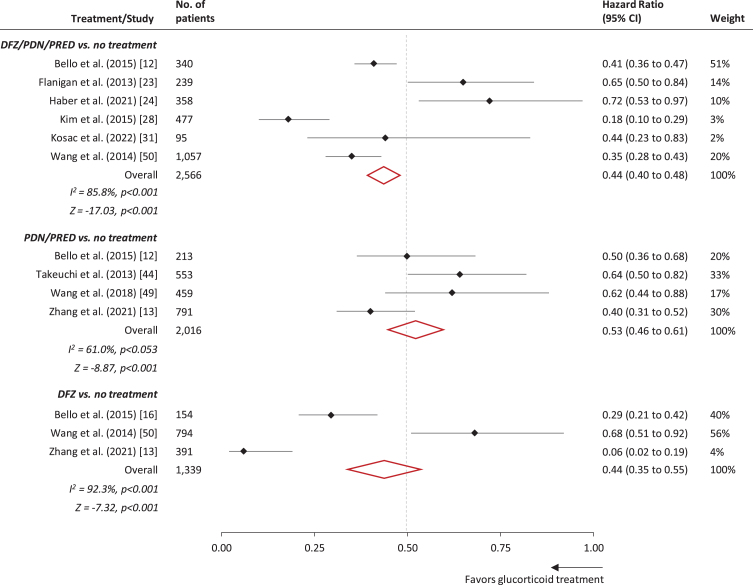
Methods: This systematic review and meta-analysis included searches of MEDLINE ALL, Embase, and the Cochrane Database of Systematic Reviews from January 1, 2000, to December 31, 2022, for predictors of loss of ambulation in DMD. Search terms included "Duchenne muscular dystrophy" as a Medical Subject Heading or free text term, in combination with variations of the term "predictor". Risk of bias was assessed using the Newcastle-Ottawa Scale. We performed meta-analysis pooling of hazard ratios of the effects of glucocorticoids (vs. no glucocorticoid therapy) by fitting a common-effect inverse-variance model.
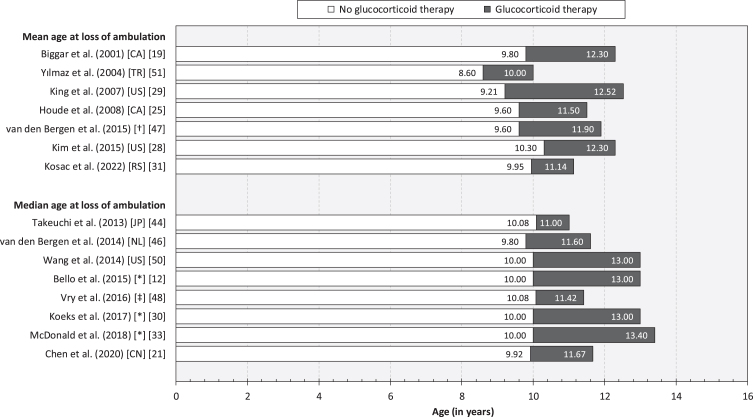
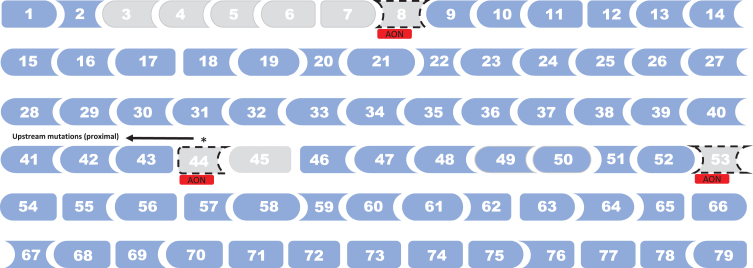
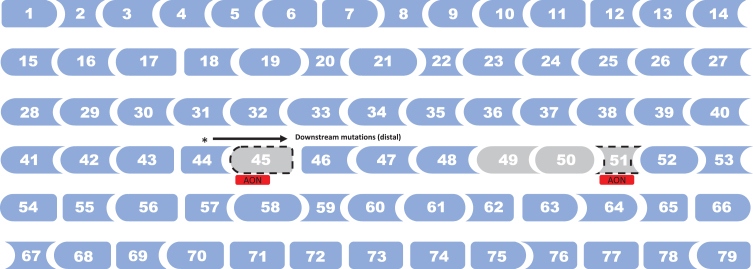
Results: The bibliographic searches resulted in the inclusion of 45 studies of children and adults with DMD from 17 countries across Europe, Asia, and North America. Glucocorticoid therapy was associated with delayed loss of ambulation (overall meta-analysis HR deflazacort/prednisone/prednisolone: 0.44 [95% CI: 0.40-0.48]) (n = 25 studies). Earlier onset of first signs or symptoms, earlier loss of developmental milestones, lower baseline 6MWT (i.e.,<350 vs. ≥350 metres and <330 vs. ≥330 metres), and lower baseline NSAA were associated with earlier loss of ambulation (n = 5 studies). Deletion of exons 3-7, proximal mutations (upstream intron 44), single exon 45 deletions, and mutations amenable of skipping exon 8, exon 44, and exon 53, were associated with prolonged ambulation; distal mutations (intron 44 and downstream), deletion of exons 49-50, and mutations amenable of skipping exon 45, and exon 51 were associated with earlier loss of ambulation (n = 13 studies). Specific single-nucleotide polymorphisms in CD40 gene rs1883832, LTBP4 gene rs10880, SPP1 gene rs2835709 and rs11730582, and TCTEX1D1 gene rs1060575 (n = 7 studies), as well as race/ethnicity and level of family/patient deprivation (n = 3 studies), were associated with loss of ambulation. Treatment with ataluren (n = 2 studies) and eteplirsen (n = 3 studies) were associated with prolonged ambulation. Magnetic resonance biomarkers (MRI and MRS) were identified as significant predictors of loss of ambulation (n = 6 studies). In total, 33% of studies exhibited some risk of bias.
Conclusion: Our synthesis of predictors of loss of ambulation in DMD contributes to the understanding the natural history of disease and informs the design of new trials of novel therapies targeting this heavily burdened patient population.
Keywords: 6MWT; Motor function; NOS; Neuromuscular Disease; guidelines; treatment.
Conflict of interest statement
Dr Alemán reports being sub-investigator of clinical trials in DMD sponsored by Pfizer and Reveragen, and receiving a research grant from PTC. Ms Zhang, Dr Werner, and Dr Tomazos are employees of PTC Therapeutics and may own stock/options in the company. Professor Lochmüller reports being principal investigator of clinical trials in DMD sponsored by Pfizer, PTC Therapeutics, Santhera, Sarepta, and Reveragen. Professor Kirschner reports support for clinical research and/or advisory activities from Biogen, Novartis, Roche, Sarepta, Scholarrock, PTC Therapeutics, and Pfizer. The remaining authors have no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
