

A new prediction nomogram of non-sentinel lymph node metastasis in cT1-2 breast cancer patients with positive sentinel lymph nodes
- PMID: 38671007
- PMCID: PMC11053028
- DOI: 10.1038/s41598-024-60198-0
A new prediction nomogram of non-sentinel lymph node metastasis in cT1-2 breast cancer patients with positive sentinel lymph nodes
Abstract
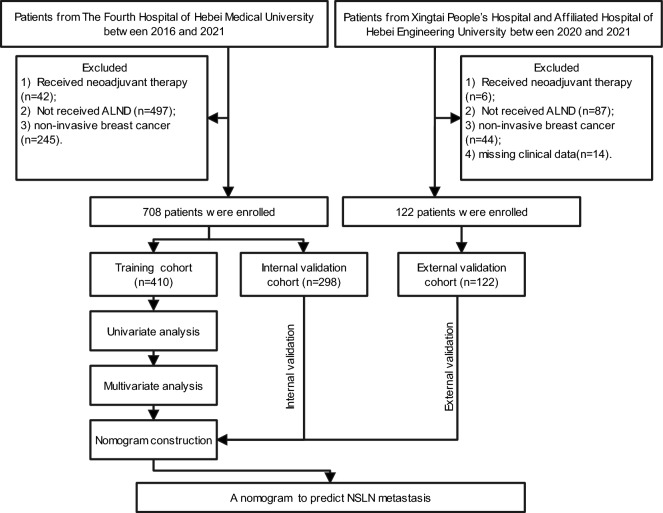
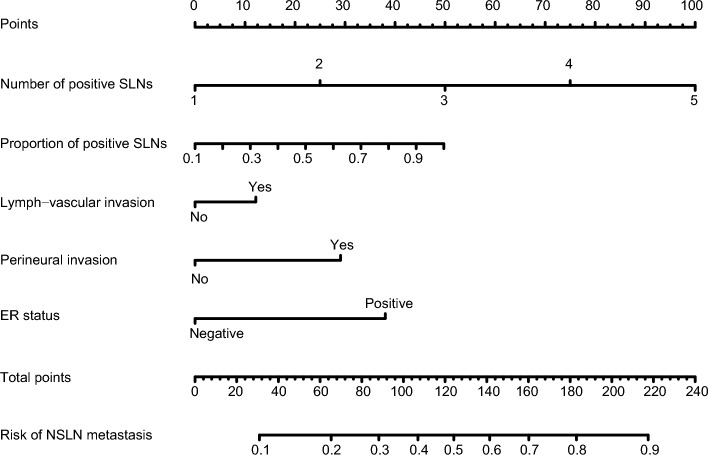
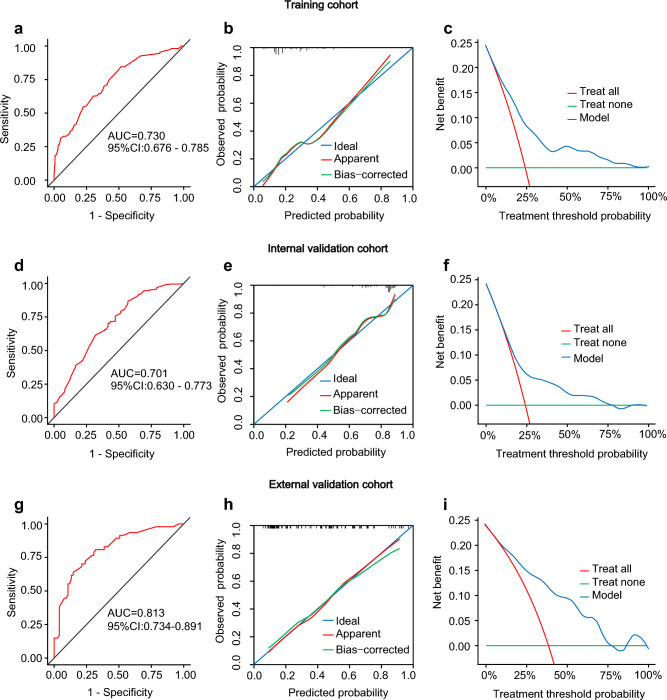
We aimed to analyze the risk factors and construct a new nomogram to predict non-sentinel lymph node (NSLN) metastasis for cT1-2 breast cancer patients with positivity after sentinel lymph node biopsy (SLNB). A total of 830 breast cancer patients who underwent surgery between 2016 and 2021 at multi-center were included in the retrospective analysis. Patients were divided into training (n = 410), internal validation (n = 298), and external validation cohorts (n = 122) based on periods and centers. A nomogram-based prediction model for the risk of NSLN metastasis was constructed by incorporating independent predictors of NSLN metastasis identified through univariate and multivariate logistic regression analyses in the training cohort and then validated by validation cohorts. The multivariate logistic regression analysis revealed that the number of positive sentinel lymph nodes (SLNs) (P < 0.001), the proportion of positive SLNs (P = 0.029), lymph-vascular invasion (P = 0.029), perineural invasion (P = 0.023), and estrogen receptor (ER) status (P = 0.034) were independent risk factors for NSLN metastasis. The area under the receiver operating characteristics curve (AUC) value of this model was 0.730 (95% CI 0.676-0.785) for the training, 0.701 (95% CI 0.630-0.773) for internal validation, and 0.813 (95% CI 0.734-0.891) for external validation cohorts. Decision curve analysis also showed that the model could be effectively applied in clinical practice. The proposed nomogram estimated the likelihood of positive NSLNs and assisted the surgeon in deciding whether to perform further axillary lymph node dissection (ALND) and avoid non-essential ALND as well as postoperative complications.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Predictive Factors for Nonsentinel Lymph Node Metastasis in Patients With Positive Sentinel Lymph Nodes After Neoadjuvant Chemotherapy: Nomogram for Predicting Nonsentinel Lymph Node Metastasis.Clin Breast Cancer. 2017 Nov;17(7):550-558. doi: 10.1016/j.clbc.2017.03.014. Epub 2017 Apr 6. Clin Breast Cancer. 2017. PMID: 28454926
-
Predicting Non-sentinel Lymph Node Metastasis in a Chinese Breast Cancer Population with 1-2 Positive Sentinel Nodes: Development and Assessment of a New Predictive Nomogram.World J Surg. 2015 Dec;39(12):2919-27. doi: 10.1007/s00268-015-3189-z. World J Surg. 2015. PMID: 26324157
-
[A nomogram to predict non-sentinel lymph node metastasis for breast cancer patients with positive axillary sentinel lymph node].Zhonghua Zhong Liu Za Zhi. 2020 Aug 23;42(8):653-659. doi: 10.3760/cma.j.cn112152-20190824-00545. Zhonghua Zhong Liu Za Zhi. 2020. PMID: 32867457 Chinese.
-
Lymphovascular invasion is a significant risk factor for non-sentinel nodal metastasis in breast cancer patients with sentinel lymph node (SLN)-positive breast cancer: a cross-sectional study.World J Surg Oncol. 2023 Dec 14;21(1):386. doi: 10.1186/s12957-023-03273-6. World J Surg Oncol. 2023. PMID: 38097994 Free PMC article. Review.
-
[AI-assisted Prediction of Lymph Node Metastasis of Breast Cancer: Current and Prospective Research].Sichuan Da Xue Xue Bao Yi Xue Ban. 2021 Mar;52(2):162-165. doi: 10.12182/20210360102. Sichuan Da Xue Xue Bao Yi Xue Ban. 2021. PMID: 33829685 Free PMC article. Review. Chinese.
Cited by
-
Identifying low-risk breast cancer patients for axillary biopsy exemption: a multimodal preoperative predictive model.Eur J Med Res. 2025 Jul 28;30(1):680. doi: 10.1186/s40001-025-02950-4. Eur J Med Res. 2025. PMID: 40717102 Free PMC article.
-
Individualized prediction of non-sentinel lymph node metastasis in Chinese breast cancer patients with ≥ 3 positive sentinel lymph nodes based on machine-learning algorithms.BMC Cancer. 2024 Sep 2;24(1):1090. doi: 10.1186/s12885-024-12870-x. BMC Cancer. 2024. PMID: 39223574 Free PMC article.
-
The prevalence of non-sentinel lymph node metastasis among breast cancer patients with sentinel lymph node involvement and its impact on clinical decision-making: a single-centred retrospective study.Oncol Rev. 2024 Oct 31;18:1495133. doi: 10.3389/or.2024.1495133. eCollection 2024. Oncol Rev. 2024. PMID: 39544961 Free PMC article.
-
Abnormal Breast Temperature and Cortical Enlargement of the Axillary Lymph Nodes Through the Thermography.Clin Case Rep. 2024 Dec 12;12(12):e9636. doi: 10.1002/ccr3.9636. eCollection 2024 Dec. Clin Case Rep. 2024. PMID: 39677871 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
