

Blood pressure and cerebral oxygenation with physiologically-based cord clamping: sub-study of the BabyDUCC trial
- PMID: 38671085
- PMCID: PMC11257956
- DOI: 10.1038/s41390-024-03131-5
Blood pressure and cerebral oxygenation with physiologically-based cord clamping: sub-study of the BabyDUCC trial
Abstract
Background: Cord-clamping strategies may modify blood pressure (BP) and cerebral tissue oxygen saturation (rStO2) immediately after birth.
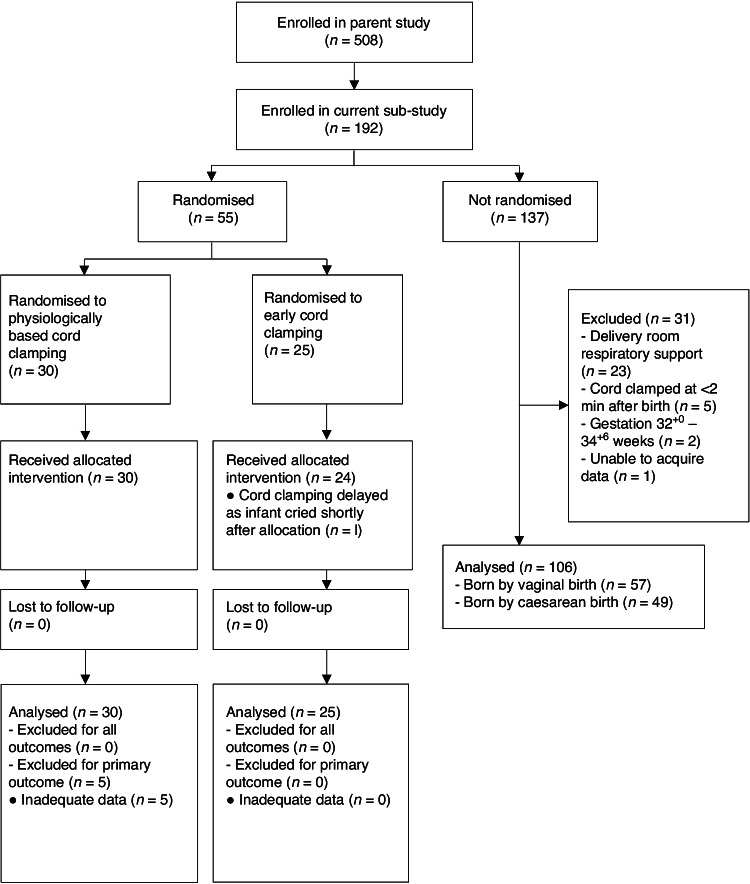
Methods: We conducted a sub-study nested within the Baby-Directed Umbilical Cord-Clamping trial. Infants ≥32+0 weeks' gestation assessed as requiring resuscitation were randomly allocated to either physiologically-based cord clamping (PBCC), where resuscitation commenced prior to umbilical cord clamping, or standard care where cord clamping occurred early (ECC). In this single-site sub-study, we obtained additional measurements of pre-ductal BP and rStO2. In a separate observational arm, non-randomised vigorous infants received 2 min of deferred cord clamping (DCC) and contributed data for reference percentiles.
Results: Among 161 included infants, n = 55 were randomly allocated to PBCC (n = 30) or ECC (n = 25). The mean (SD) BP at 3-4 min after birth (primary outcome) in the PBCC group was 64 (10) mmHg compared to 62 (10) mmHg in the ECC group, mean difference 2 mmHg (95% confidence interval -3-8 mmHg, p = 0.42). BP and rStO2 were similar across both randomised arms and the observational arm (n = 106).
Conclusion: We found no difference in BP or rStO2 with the different cord clamping strategies. We report reference ranges for BP and rStO2 for late-preterm and full-term infants receiving DCC.
Impact: Among late-preterm and full-term infants receiving varying levels of resuscitation, blood pressure (BP, at 3-4 minutes and 6 min) and cerebral tissue oxygen saturation (rStO2) are not influenced by timing of cord clamping in relation to establishment of ventilation. Infants in this study did not require advanced resuscitation, where cord clamping strategies may yet influence BP and rStO2. The reference ranges for BP and rStO2 represent the first, to our knowledge, for vigorous late-preterm and full-term infants receiving deferred cord clamping. rStO2 > 90% (~90th percentile) may be used to define cerebral hyperoxia, for instance when studying oxygen supplementation after birth.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
