

The association of the perioperative fluid balance and cardiopulmonary complications in emergency gastrointestinal surgery: exploration of a randomized trial
- PMID: 38671528
- PMCID: PMC11055263
- DOI: 10.1186/s13741-024-00390-y
The association of the perioperative fluid balance and cardiopulmonary complications in emergency gastrointestinal surgery: exploration of a randomized trial
Abstract
Background: The association between perioperative fluid administration and risk of complications following emergency surgery is poorly studied. We tested the association between the perioperative fluid balance and postoperative complications following emergency surgery for gastrointestinal obstruction or perforation.
Methods: We performed a re-assessment of data from the Goal-directed Fluid Therapy in Urgent Gastrointestinal Surgery Trial (GAS-ART) studying intra-operative stroke volume optimization and postoperative zero-balance fluid therapy versus standard fluid therapy. The cohort was divided into three groups at a perioperative fluid balance (FB) of low < 0 L, moderate 0-2 L, or high > 2 L. We used a propensity adjusted logistic regression to analyse the association with cardiopulmonary (primary outcome), renal, infectious, and wound healing complications. Further, the risk of complications was explored on a continuous scale of the FB.
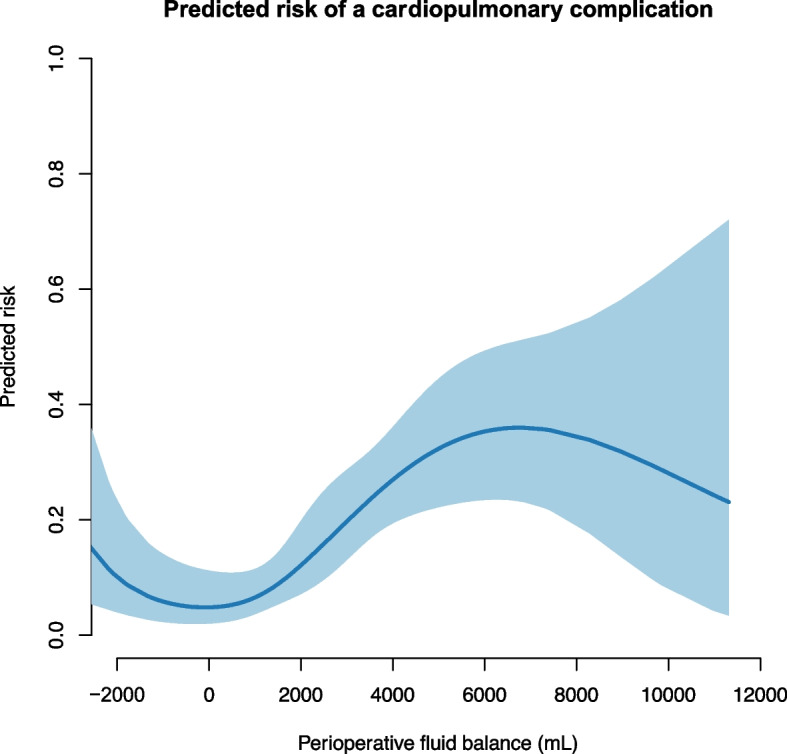
Results: We included 303 patients: 44 patients belonged to the low-FB group, 108 to the moderate-FB group, and 151 to the high-FB group. The median [interquartile range] perioperative FB was -0.9 L [-1.4, -0.6], 0.9 L [0.5, 1.3], and 3.8 L [2.7, 5.3]. The risk of cardiopulmonary complications was significantly higher in the High-FB group 3.4 (1.5-7.6), p = 0.002 (odds ratio (95% confidence interval). On a continuous scale of the fluid balance, the risk of cardiopulmonary complications was minimal at -1 L to 1 L.
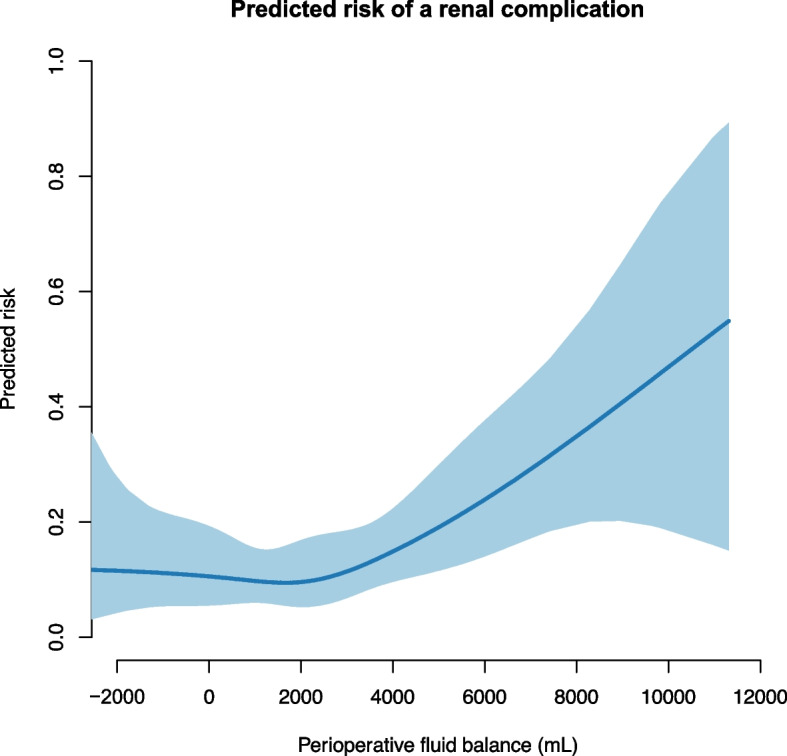
Conclusion: Following emergency surgery for gastrointestinal obstruction or perforation, a fluid balance < 2.0 L was associated with decreased risk of cardiopulmonary complications without increasing renal complications.
Keywords: Fluid therapy; Intestinal obstruction; Intestinal perforation; Intraoperative care; Postoperative complications; Prospective study.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Becher RD, Hoth JJ, Miller PR, Mowery NT, Chang MC, Meredith JW. A critical assessment of outcomes in emergency versus nonemergency general surgery using the American College of Surgeons National Surgical Quality Improvement Program database. Am Surg. 2011;77(7):951–959. doi: 10.1177/000313481107700738. - DOI - PubMed
-
- Brandstrup B, Tønnesen H, Beier-Holgersen R, et al. Effects of intravenous fluid restriction on postoperative complications: comparison of two perioperative fluid regimens: a randomized assessor-blinded multicenter trial. Ann Surg. 2003;238(5):641–648. doi: 10.1097/01.sla.0000094387.50865.23. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
