

Prognostic nutritional index as a predictive marker for acute kidney injury in adult critical illness population: a systematic review and diagnostic test accuracy meta-analysis
- PMID: 38671543
- PMCID: PMC11046764
- DOI: 10.1186/s40560-024-00729-z
Prognostic nutritional index as a predictive marker for acute kidney injury in adult critical illness population: a systematic review and diagnostic test accuracy meta-analysis
Abstract
Background: The prognostic nutritional index (PNI), integrating nutrition and inflammation markers, has been increasingly recognized as a prognostic predictor in diverse patient cohorts. Recently, its effectiveness as a predictive marker for acute kidney injury (AKI) in various clinical settings has gained attention. This study aims to assess the predictive accuracy of the PNI for AKI in critically ill populations through systematic review and meta-analysis.
Methods: A systematic review was conducted using the databases MEDLINE, EMBASE, PubMed, and China National Knowledge Infrastructure up to August 2023. The included trials reported the PNI assessment in adult population with critical illness and its predictive capacity for AKI. Data on study characteristics, subgroup covariates, and diagnostic performance of PNI, including sensitivity, specificity, and event rates, were extracted. A diagnostic test accuracy meta-analysis was performed. Subgroup analyses and meta-regression were utilized to investigate the sources of heterogeneity. The GRADE framework evaluated the confidence in the meta-analysis's evidence.
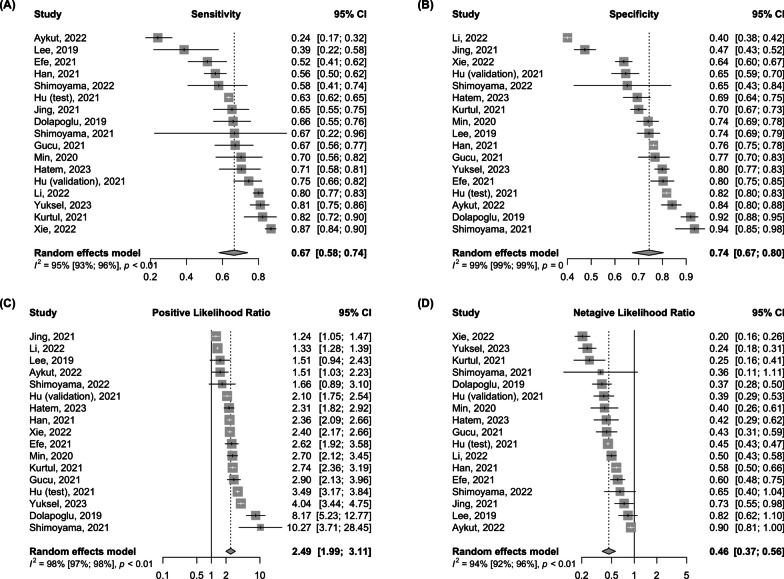
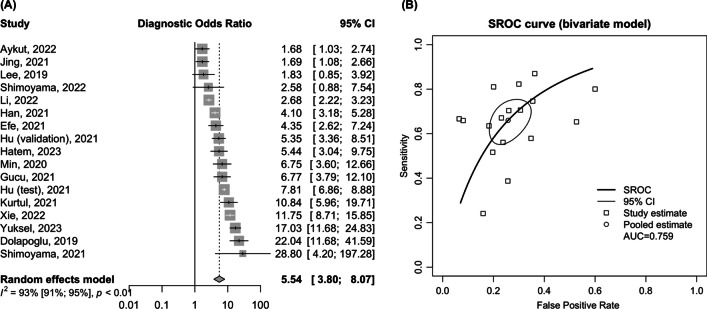
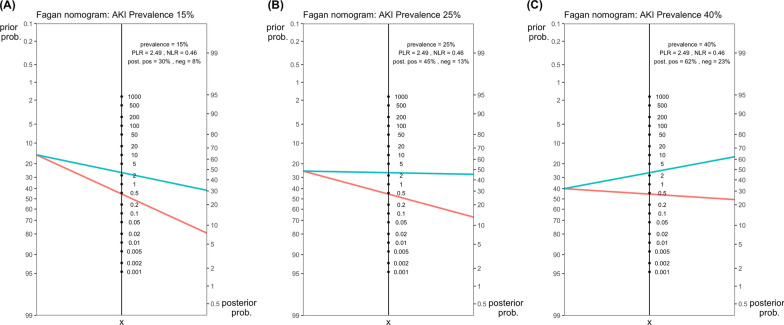
Results: The analysis encompassed 16 studies with 17 separate cohorts, totaling 21,239 patients. The pooled sensitivity and specificity of PNI for AKI prediction were 0.67 (95% CI 0.58-0.74) and 0.74 (95% CI 0.67-0.80), respectively. The pooled positive likelihood ratio was 2.49 (95% CI 1.99-3.11; low certainty), and the negative likelihood ratio was 0.46 (95% CI 0.37-0.56; low certainty). The pooled diagnostic odds ratio was 5.54 (95% CI 3.80-8.07), with an area under curve of summary receiver operating characteristics of 0.76. Subgroup analysis showed that PNI's sensitivity was higher in medical populations than in surgical populations (0.72 vs. 0.55; p < 0.05) and in studies excluding patients with chronic kidney disease (CKD) than in those including them (0.75 vs. 0.56; p < 0.01). Overall, diagnostic performance was superior in the non-chronic kidney disease group.
Conclusion: Our study demonstrated that PNI has practical accuracy for predicting the development of AKI in critically ill populations, with superior diagnostic performance observed in medical and non-CKD populations. However, the diagnostic efficacy of the PNI has significant heterogeneity with different cutoff value, indicating the need for further research.
Keywords: Acute kidney injury; Meta-analysis; Prognostic nutritional index; Risk.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Tsai TT, Patel UD, Chang TI, et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the NCDR Cath-PCI registry. JACC Cardiovasc Interv. 2014;7(1):1–9. doi: 10.1016/j.jcin.2013.06.016. - DOI - PMC - PubMed
-
- Warren J, Mehran R, Baber U, et al. Incidence and impact of acute kidney injury in patients with acute coronary syndromes treated with coronary artery bypass grafting: insights from the Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI) and Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trials. Am Heart J. 2016;171(1):40–47. doi: 10.1016/j.ahj.2015.07.001. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
