

A Second Trimester Prediction Algorithm for Early-Onset Hypertensive Disorders of Pregnancy Occurrence and Severity Based on Soluble fms-like Tyrosine Kinase 1 (sFlt-1)/Placental Growth Factor (PlGF) Ratio and Uterine Doppler Ultrasound in Women at Risk
- PMID: 38671685
- PMCID: PMC11049313
- DOI: 10.3390/children11040468
A Second Trimester Prediction Algorithm for Early-Onset Hypertensive Disorders of Pregnancy Occurrence and Severity Based on Soluble fms-like Tyrosine Kinase 1 (sFlt-1)/Placental Growth Factor (PlGF) Ratio and Uterine Doppler Ultrasound in Women at Risk
Abstract
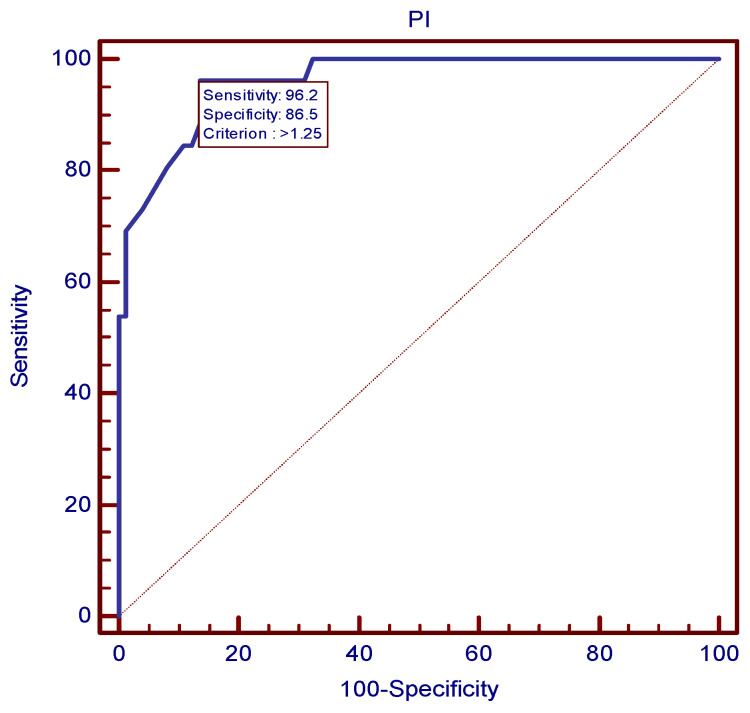
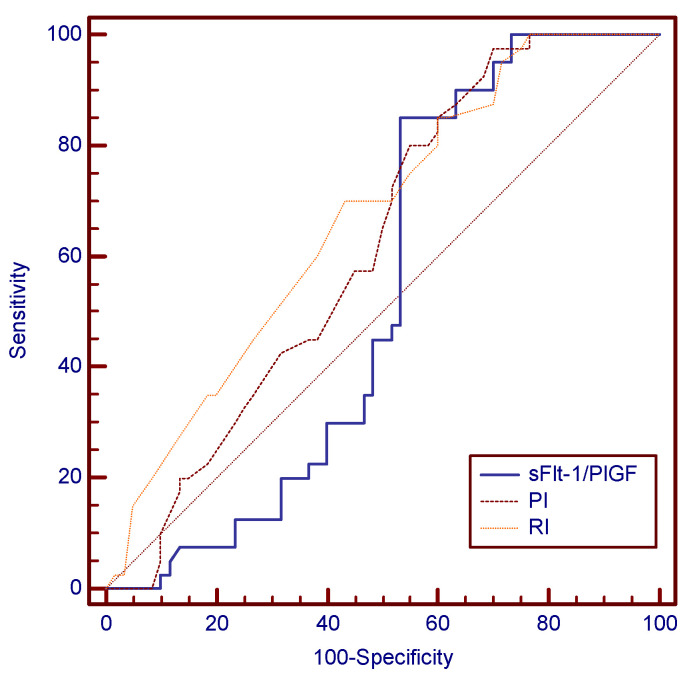
Hypertensive disorders of pregnancy (HDPs) represent a significant source of severe maternal and fetal morbidity. Screening strategies relying on traditional medical history and clinical risk factors have traditionally shown relatively modest performance, mainly in the prediction of preeclampsia, displaying a sensitivity of 37% for the early-onset form and 29% for the late-onset form. The development of more accurate predictive and diagnostic models of preeclampsia in the early stages of pregnancy represents a matter of high priority. The aim of the present paper is to create an effective second trimester prediction algorithm of early-onset HDP occurrence and severity, by combining the following two biochemical markers: a soluble fms-like tyrosine kinase 1 (sFlt-1)/placental growth factor (PlGF) ratio and uterine artery Doppler ultrasound parameters, namely the pulsatility index (PI) and the resistivity index (RI), in a population of high-risk pregnant women, initially assessed through traditional risk factors. A prospective single-center observational longitudinal study was conducted, in which 100 women with singleton pregnancy and traditional clinical and medical history risk factors for preeclampsia were enrolled at 24 weeks of gestation. Shortly after study enrollment, all women had their sFlt-1 and PlGF levels and mean uterine artery PI and RI determined. All pregnancies were followed up until delivery. Receiver operating characteristic (ROC) analysis established algorithms based on cutoffs for the prediction of the later development of preeclampsia: PI 1.25 (96.15% sensitivity, 86.49% specificity), RI 0.62 (84.6% sensitivity, 89.2% specificity) and sFlt-1/PlGF ratio 59.55 (100% sensitivity, 89.2% specificity). The sFlt-1/PlGF ratio was the best predictor for preeclampsia, as it displayed the highest area under the curve (AUC) of 0.973. The prediction algorithm for the severe form of preeclampsia, complicated by fetal growth restriction leading to preterm birth, antepartum fetal demise or acute fetal distress with a cerebro-placental ratio of <one consisted of the following cutoffs: PI 1.44 (93.75% sensitivity, 95.24% specificity), RI 0.69 (87.5% sensitivity, 100% specificity) and sFlt-1/PlGF ratio 102.74 (93.75% sensitivity, 95.2% specificity). These algorithms may significantly enhance the prediction accuracy of preeclampsia compared to traditional risk factors. The combination of the sFlt-1/PlGF ratio with mean uterine PI and RI in particular displayed an improved performance in the prediction of severe preeclampsia with the above-mentioned complications, compared to the biochemical markers or uterine Doppler parameters used alone. Therefore, HDP screening strategies should increasingly focus on implementing such algorithms for women who are initially regarded as high risk based on traditional risk factors, in order to properly diagnose HDP and properly limit or manage the later maternal and fetal complications.
Keywords: gestational hypertension; intrauterine growth restriction; prediction; preeclampsia; soluble fms-like tyrosine kinase 1 (sFlt-1)/placental growth factor (PlGF) ratio; uterine Doppler.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







References
-
- Garovic V.D., Dechend R., Easterling T., Karumanchi S.A., McMurtry Baird S., Magee L.A., Rana S., Vermunt J.V., August P., American Heart Association Council on Hypertension et al. Hypertension in Pregnancy: Diagnosis, Blood Pressure Goals, and Pharmacotherapy: A Scientific Statement From the American Heart Association. Hypertension. 2022;79:e21–e41. doi: 10.1161/HYP.0000000000000208. Erratum in Hypertension 2022, 79, e70. - DOI - PMC - PubMed
-
- Brown M.A., Magee L.A., Kenny L.C., Karumanchi S.A., McCarthy F.P., Saito S., Hall D.R., Warren C.E., Adoyi G., Ishaku S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018;13:291–310. - PubMed
-
- Espinoza J., Vidaeff A., Pettker C.M., Simhan H. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet Gynecol. 2020;135:e237–e260. - PubMed
-
- Unger T., Borghi C., Charchar F., Khan N.A., Poulter N.R., Prabhakaran D., Ramirez A., Schlaich M., Stergiou G.S., Tomaszewski M., et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension. 2020;75:1334–1357. doi: 10.1161/HYPERTENSIONAHA.120.15026. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
