

Dual-Time-Point 18F-FDG PET/CT in Infective Endocarditis: Impact of Delayed Imaging in the Definitive Diagnosis of Endocarditis
- PMID: 38672215
- PMCID: PMC11048229
- DOI: 10.3390/biomedicines12040861
Dual-Time-Point 18F-FDG PET/CT in Infective Endocarditis: Impact of Delayed Imaging in the Definitive Diagnosis of Endocarditis
Abstract
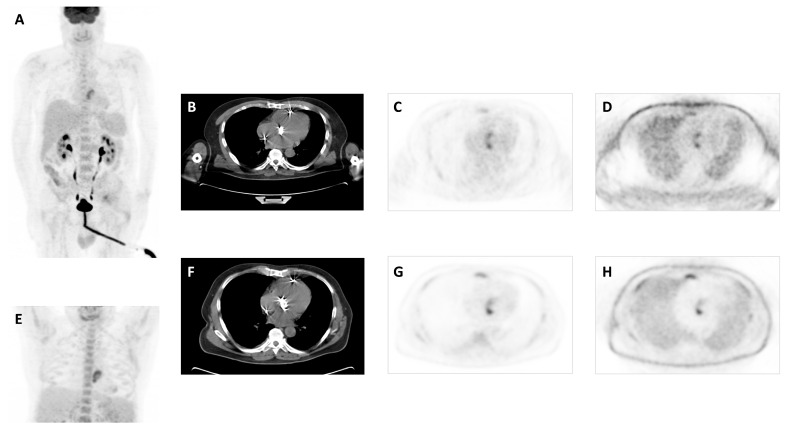
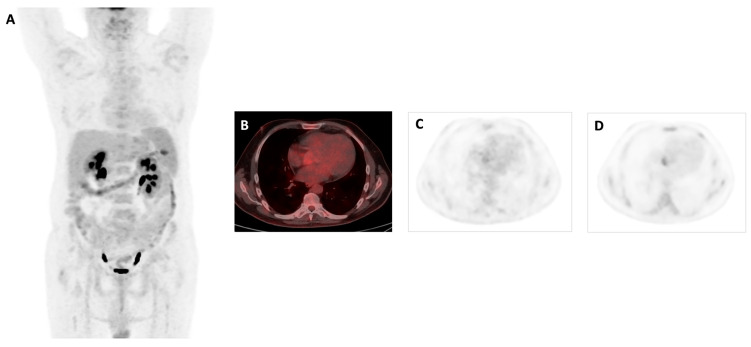
Infective endocarditis (IE) is a major public health condition due to the associated high morbidity and mortality. Our objective was to evaluate the utility of dual-time 2-deoxy-2-[18F] fluoro-D-glucose (18F-FDG) Positron Emission Tomography/Computed Tomography (PET/CT) imaging in the diagnosis of active IE in patients with suspected native valve endocarditis (NVE) and prosthetic valve endocarditis (PVE). For this purpose, a retrospective study was carried out, including patients suspicious of NVE or PVE who underwent a dual-time-point 18F-FDG PET/CT. A final diagnosis was established by the Endocarditis Team after patient follow-up using all the available findings. Sixty-nine patients were assessed. A final diagnosis of NVE was established in 3 patients of the 34 by 18F-FDG PET/CT and in the case of PVE was established in 20 patients of the 35. A statistically significant association was found when evaluating the association between PET diagnosis at early acquisition and final diagnosis of IE (χ2 = 30.198, p < 0.001) and PET diagnosis at delayed acquisition for final diagnosis of IE (χ2 = 9.412, p = 0.002). Delayed PET/CT imaging determined the IE diagnosis in 16/58 of the studies. In conclusion, delayed 18F-FDG PET/CT imaging seems to be useful in improving the definitive diagnosis of IE.
Keywords: PET/CT; dual-time-point; infective endocarditis; native valve; prosthetic valve.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
The Role of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Diagnosis of Left-sided Endocarditis: Native vs Prosthetic Valves Endocarditis.Clin Infect Dis. 2020 Feb 3;70(4):583-594. doi: 10.1093/cid/ciz267. Clin Infect Dis. 2020. PMID: 30949690
-
18-Fluoro-2-deoxyglucose positron emission tomography-computed tomography: an additional tool in the diagnosis of prosthetic valve endocarditis.Int J Infect Dis. 2014 Nov;28:219-24. doi: 10.1016/j.ijid.2014.04.028. Epub 2014 Aug 2. Int J Infect Dis. 2014. PMID: 25093540
-
18F-FDG positron emission tomography/computed tomography in infective endocarditis.J Nucl Cardiol. 2017 Feb;24(1):195-206. doi: 10.1007/s12350-015-0325-y. Epub 2015 Dec 9. J Nucl Cardiol. 2017. PMID: 26662063
-
Detection of Native and Prosthetic Valve Endocarditis: Incremental Attributes of Functional FDG PET/CT over Morphologic Imaging.Curr Cardiol Rep. 2020 Jul 9;22(9):93. doi: 10.1007/s11886-020-01334-w. Curr Cardiol Rep. 2020. PMID: 32647931 Review.
-
The additional role of 18F-FDG PET/CT in prosthetic valve endocarditis.Eur Rev Med Pharmacol Sci. 2018 Mar;22(6):1744-1751. doi: 10.26355/eurrev_201803_14590. Eur Rev Med Pharmacol Sci. 2018. PMID: 29630121 Review.
Cited by
-
Distinguishing benign lesions from malignant ones using FAPI-based tracers: will we need to bid farewell to dual-time points imaging?Eur J Nucl Med Mol Imaging. 2025 Apr 9. doi: 10.1007/s00259-025-07254-7. Online ahead of print. Eur J Nucl Med Mol Imaging. 2025. PMID: 40202685 No abstract available.
-
Diagnostic Utility of 18F-FDG PET/CT in Infective Endocarditis.Microorganisms. 2025 Jun 3;13(6):1299. doi: 10.3390/microorganisms13061299. Microorganisms. 2025. PMID: 40572187 Free PMC article.
References
-
- Institute for Health Metrics Evaluation GPllobal Burden of Disease Metrics. University of Washington, Seattle. [(accessed on 1 October 2021)]. Available online: https://vizhub.healthdata.org/gbd-compare/
-
- Momtazmanesh S., Saeedi Moghaddam S., Malakan Rad E., Azadnajafabad S., Ebrahimi N., Mohammadi E., Rouhifard M., Rezaei N., Masinaei M., Rezaei N., et al. Global, Regional, and National Burden and Quality of Care Index of Endocarditis: The Global Burden of Disease Study 1990–2019. Eur. J. Prev. Cardiol. 2022;29:1287–1297. doi: 10.1093/eurjpc/zwab211. - DOI - PubMed
-
- Heredia-Rodríguez M., Hernández A., Bustamante-Munguira J., Álvarez F.J., Eiros J.M., Castrodeza J., Tamayo E. Evolution of the Incidence, Mortality, and Cost of Infective Endocarditis in Spain Between 1997 and 2014. J. Gen. Intern. Med. 2018;33:1610–1613. doi: 10.1007/s11606-018-4514-7. - DOI - PMC - PubMed
-
- Jensen A.D., Bundgaard H., Butt J.H., Bruun N.E., Voldstedlund M., Torp-Pedersen C., Gislason G., Iversen K., Chamat S., Dahl A., et al. Temporal Changes in the Incidence of Infective Endocarditis in Denmark 1997–2017: A Nationwide Study. Int. J. Cardiol. 2021;326:145–152. doi: 10.1016/j.ijcard.2020.10.029. - DOI - PubMed
-
- Van Den Brink F.S., Swaans M.J., Hoogendijk M.G., Alipour A., Kelder J.C., Jaarsma W., Eefting F.D., Groenmeijer B., Kupper A.J.F., Ten Berg J.M. Increased Incidence of Infective Endocarditis after the 2009 European Society of Cardiology Guideline Update: A Nationwide Study in the Netherlands. Eur. Heart J. Qual. Care Clin. Outcomes. 2017;3:141–147. doi: 10.1093/ehjqcco/qcw039. - DOI - PubMed
LinkOut - more resources
Full Text Sources
