

Elevated Serum Xanthine Oxidase and Its Correlation with Antioxidant Status in Patients with Parkinson's Disease
- PMID: 38672506
- PMCID: PMC11048637
- DOI: 10.3390/biom14040490
Elevated Serum Xanthine Oxidase and Its Correlation with Antioxidant Status in Patients with Parkinson's Disease
Abstract
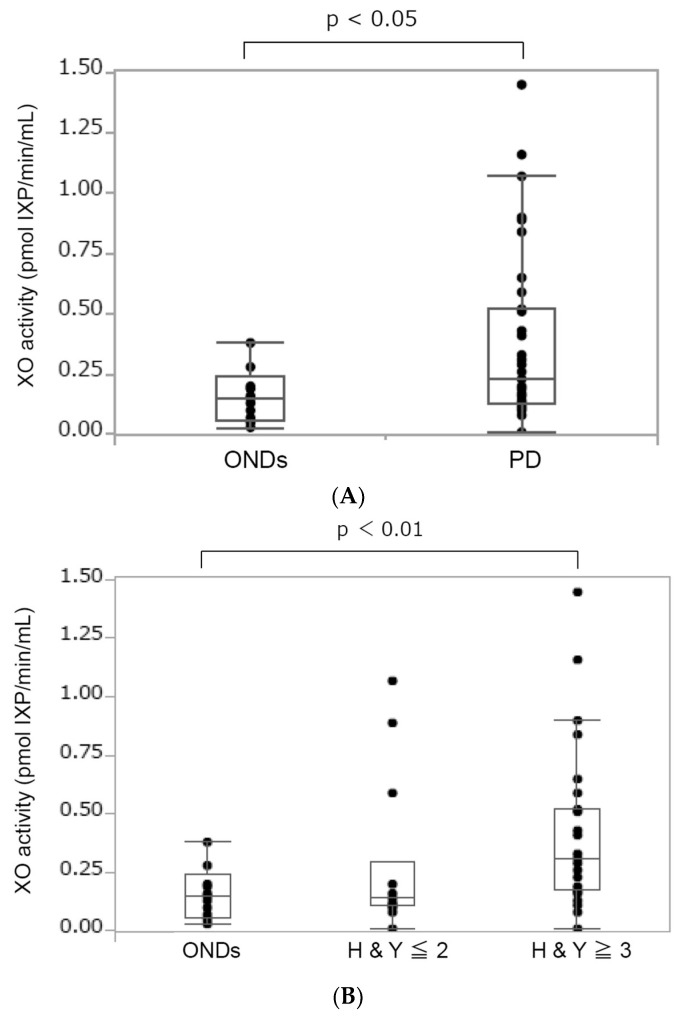
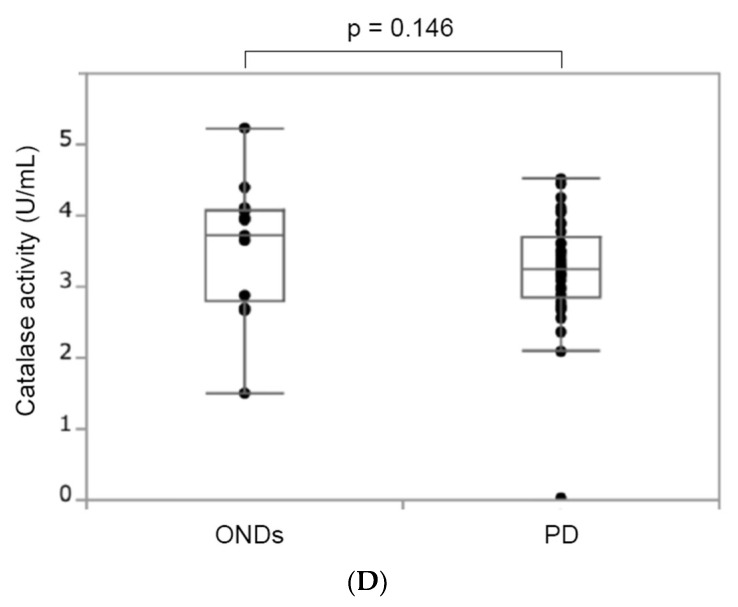
Parkinson's disease (PD) is a neurodegenerative movement disorder associated with a loss of dopamine neurons in the substantia nigra. The diagnosis of PD is sensitive since it shows clinical features that are common with other neurodegenerative diseases. In addition, most symptoms arise at the late stage of the disease, where most dopaminergic neurons are already damaged. Several studies reported that oxidative stress is a key modulator in the development of PD. This condition occurs due to excess reactive oxygen species (ROS) production in the cellular system and the incapability of antioxidants to neutralize it. In this study, we focused on the pathology of PD by measuring serum xanthine oxidase (XO) activity, which is an enzyme that generates ROS. Interestingly, the serum XO activity of patients with PD was markedly upregulated compared to patients with other neurological diseases (ONDs) as a control. Moreover, serum XO activity in patients with PD showed a significant correlation with the disease severity based on the Hoehn and Yahr (HY) stages. The investigation of antioxidant status also revealed that serum uric acid levels were significantly lower in the severe group (HY ≥ 3) than in the ONDs group. Together, these results suggest that XO activity may contribute to the development of PD and might potentially be a biomarker for determining disease severity in patients with PD.
Keywords: Parkinson’s disease; oxidative stress; xanthine oxidase.
Conflict of interest statement
Author Takashi Shirakura and Chieko Matsui are employed by the company Teijin Pharma Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Serum glutathione peroxidase, xanthine oxidase, and superoxide dismutase activities and malondialdehyde levels in patients with Parkinson's disease.Neurol Sci. 2017 Mar;38(3):425-431. doi: 10.1007/s10072-016-2782-8. Epub 2016 Nov 30. Neurol Sci. 2017. PMID: 27900485
-
Serum level of Xanthine oxidase, Uric Acid, and NADPH oxidase1 in Stage I of Multiple Myeloma.Asian Pac J Cancer Prev. 2020 Aug 1;21(8):2237-2242. doi: 10.31557/APJCP.2020.21.8.2237. Asian Pac J Cancer Prev. 2020. PMID: 32856850 Free PMC article.
-
Lower Serum Bilirubin and Uric Acid Concentrations in Patients with Parkinson's Disease in China.Cell Biochem Biophys. 2015 May;72(1):49-56. doi: 10.1007/s12013-014-0402-x. Cell Biochem Biophys. 2015. PMID: 25449297
-
Oxidative stress and Parkinson's disease: conflict of oxidant-antioxidant systems.Neurosci Lett. 2019 Sep 14;709:134296. doi: 10.1016/j.neulet.2019.134296. Epub 2019 May 30. Neurosci Lett. 2019. PMID: 31153970 Review.
-
Urate in Parkinson's disease: more than a biomarker?Curr Neurol Neurosci Rep. 2012 Aug;12(4):367-75. doi: 10.1007/s11910-012-0282-7. Curr Neurol Neurosci Rep. 2012. PMID: 22580741 Review.
Cited by
-
Xanthine Oxidoreductase: A Double-Edged Sword in Neurological Diseases.Antioxidants (Basel). 2025 Apr 17;14(4):483. doi: 10.3390/antiox14040483. Antioxidants (Basel). 2025. PMID: 40298821 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
