

Association of Fetal Lung Development Disorders with Adult Diseases: A Comprehensive Review
- PMID: 38672994
- PMCID: PMC11051200
- DOI: 10.3390/jpm14040368
Association of Fetal Lung Development Disorders with Adult Diseases: A Comprehensive Review
Abstract
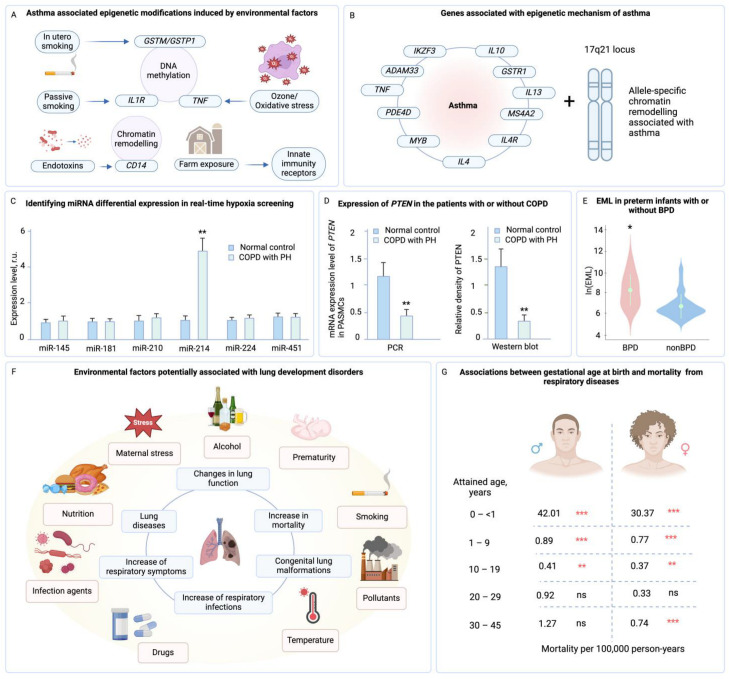
Fetal lung development is a crucial and complex process that lays the groundwork for postnatal respiratory health. However, disruptions in this delicate developmental journey can lead to fetal lung development disorders, impacting neonatal outcomes and potentially influencing health outcomes well into adulthood. Recent research has shed light on the intriguing association between fetal lung development disorders and the development of adult diseases. Understanding these links can provide valuable insights into the developmental origins of health and disease, paving the way for targeted preventive measures and clinical interventions. This review article aims to comprehensively explore the association of fetal lung development disorders with adult diseases. We delve into the stages of fetal lung development, examining key factors influencing fetal lung maturation. Subsequently, we investigate specific fetal lung development disorders, such as respiratory distress syndrome (RDS), bronchopulmonary dysplasia (BPD), congenital diaphragmatic hernia (CDH), and other abnormalities. Furthermore, we explore the potential mechanisms underlying these associations, considering the role of epigenetic modifications, transgenerational effects, and intrauterine environmental factors. Additionally, we examine the epidemiological evidence and clinical findings linking fetal lung development disorders to adult respiratory diseases, including asthma, chronic obstructive pulmonary disease (COPD), and other respiratory ailments. This review provides valuable insights for healthcare professionals and researchers, guiding future investigations and shaping strategies for preventive interventions and long-term care.
Keywords: adult respiratory diseases; epigenetic modifications; fetal respiratory diseases; lung development; neonatal outcomes; preventive interventions; transgenerational effects.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







References
-
- He P., Lim K., Sun D., Pett J.P., Jeng Q., Polanski K., Dong Z., Bolt L., Richardson L., Mamanova L., et al. A Human Fetal Lung Cell Atlas Uncovers Proximal-Distal Gradients of Differentiation and Key Regulators of Epithelial Fates. Cell. 2022;185:4841–4860.e25. doi: 10.1016/j.cell.2022.11.005. - DOI - PubMed
-
- Cao S., Feng H., Yi H., Pan M., Lin L., Zhang Y.S., Feng Z., Liang W., Cai B., Li Q., et al. Single-Cell RNA Sequencing Reveals the Developmental Program Underlying Proximal–Distal Patterning of the Human Lung at the Embryonic Stage. Cell Res. 2023;33:421–433. doi: 10.1038/s41422-023-00802-6. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
