

Review
doi: 10.3390/jpm14040407.
Role of Cardiovascular Magnetic Resonance in Cardiac Amyloidosis: A Narrative Review
Affiliations
- PMID: 38673034
- PMCID: PMC11051560
- DOI: 10.3390/jpm14040407
Item in Clipboard
Review
Role of Cardiovascular Magnetic Resonance in Cardiac Amyloidosis: A Narrative Review
J Pers Med.
.
Abstract
Amyloidosis is a rare infiltrative condition resulting from the extracellular accumulation of amyloid fibrils at the cardiac level. It can be an acquired condition or due to genetic mutations. With the progression of imaging technologies, a non-invasive diagnosis was proposed. In this study, we discuss the role of CMR in cardiac amyloidosis, focusing on the two most common subtypes (AL and ATTR), waiting for evidence-based guidelines to be published.
Keywords: T1 mapping; T2 mapping; cardiac amyloidosis (CA); cardiovascular magnetic resonance (CMR); extracellular volume (ECV); late gadolinium enhancement (LGE).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
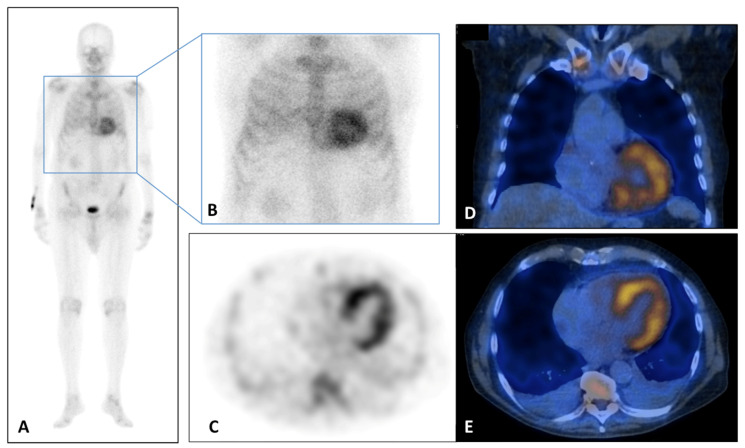
(A–E) 99Tc-Sn-HDP Scintigraphy performed in a 80 years old man with suspicious of cardiac amyloidosis and absent monoclonal protein. He presented to the emergency department for lipothymia and echocardiogram demonstrated signs of infiltrative cardiomyopathy with a LVEF of 40%, global longitudinal LV strain of −18% in absolute value. In addition, laboratory testing was significant for N-terminal pro b-type natriuretic peptide (NT-ProBNP) elevation at 5053 pg/mL (n.v. < 127.4 pg/mL). Whole Body (A) and static (B) planar bone scintigraphy, completed with tomographic imaging SPET (axial, (C)) and hybrid SPET/CT (coronal, (B) and axial, (C)) demonstrated moderate cardiac uptake. It correlated with score 2 of Perugini grading scale (cardiac uptake with intensity similar rib uptake), confirming the TTR amyloidosis diagnosis. LV, left ventricle; LVEF, left ventricular ejection fraction; NT-ProBNP, N-terminal pro b-type natriuretic peptide.
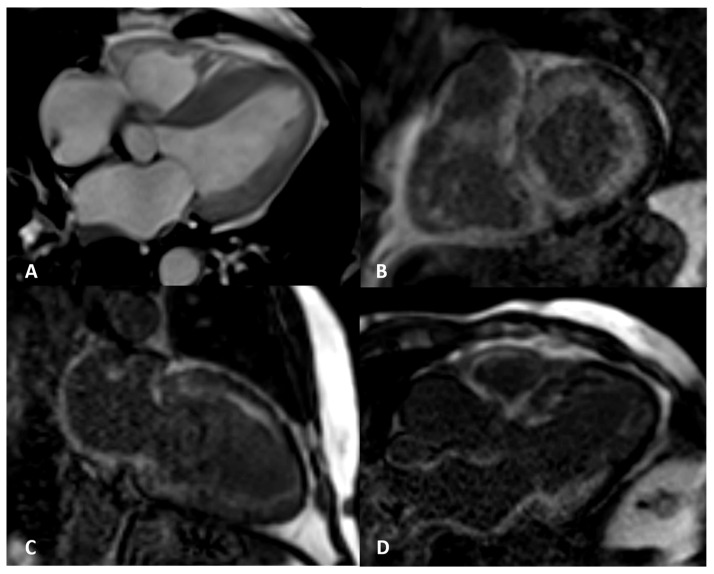
AL amyloidosis confirmed by endomyocardial biopsy. An elderly patient with NYHA III heart failure and 42% LVEF. Four-chamber balanced-steady state free precession (b-SSFP) MRI (A) shows symmetric thickening of the left ventricle with the septum maximally measuring 25 mm. Circumferential subendocardial LV LGE in two-chamber short (B) and long axes (C) and three-chamber b-SSFP (D); QALE score 12.
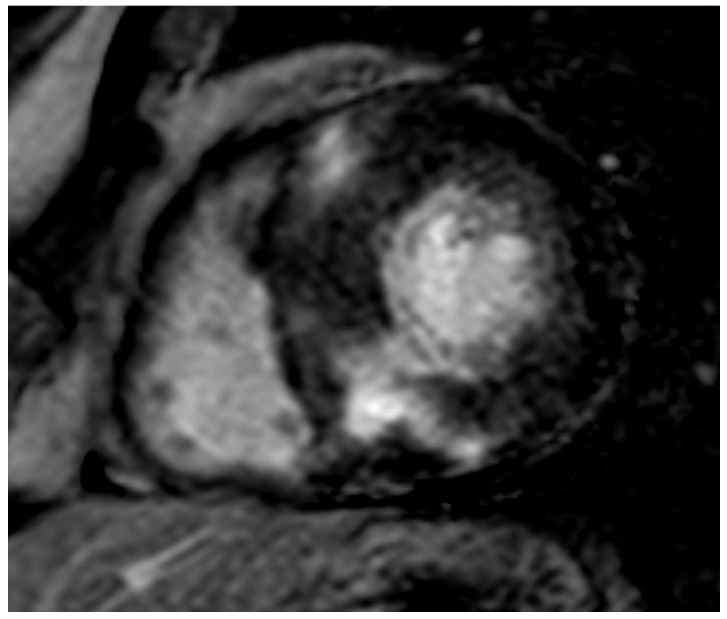
ATTR elderly patient. Transmural semicircumferential LGE pattern and symmetric thickening of the left ventricle with septum maximally measuring 21 mm.
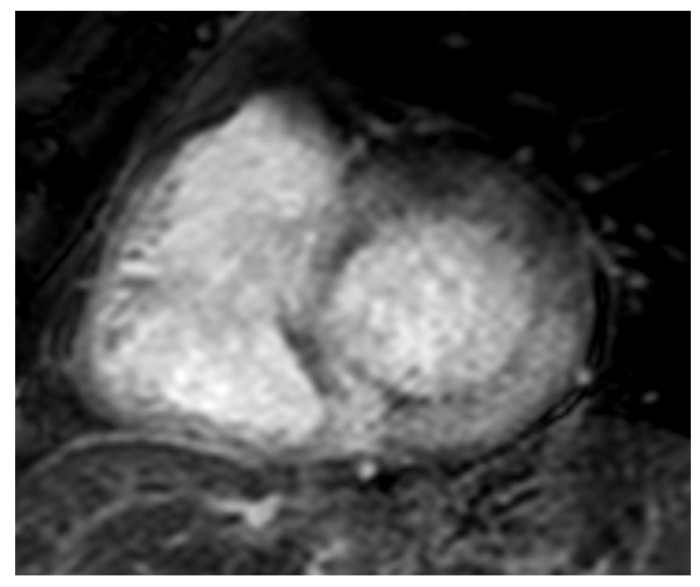
AL 68-year-old patient diagnosed with endomyocardial biopsy. T1 scout sequence shows abnormal contrast agent kinetics (Dark blood pool signal).
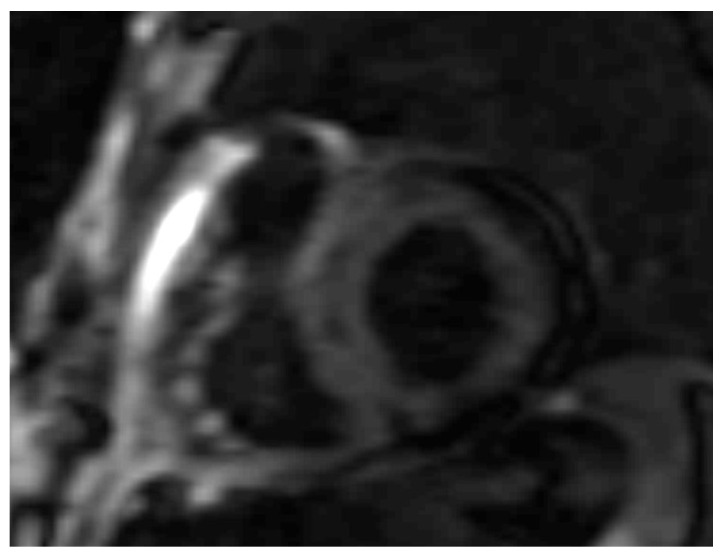
AL 64-year-old patient diagnosed with endomyocardial biopsy. PSIR sequence highlights transmural patchy LGE pattern.
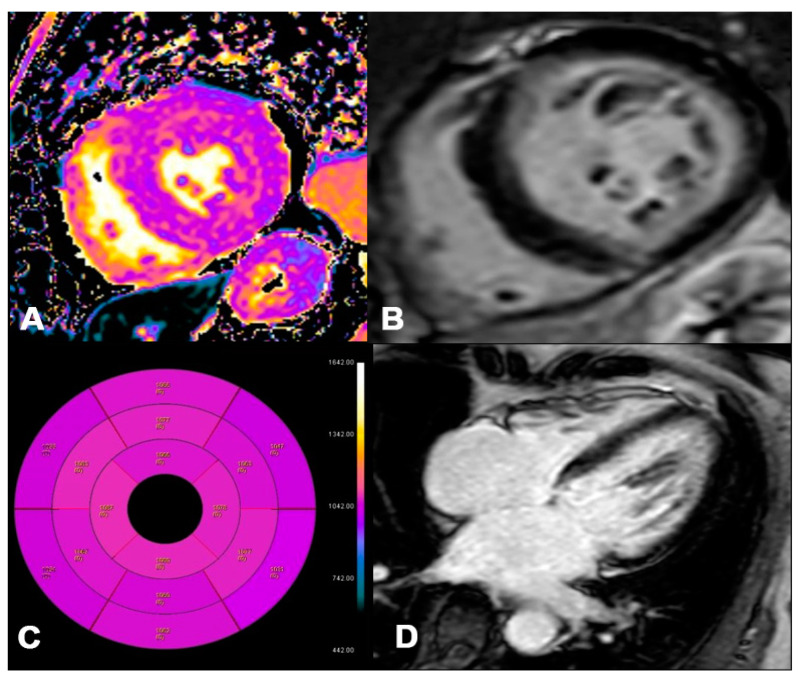
AL 73-year-old patient diagnosed with endomyocardial biopsy. T1 Native Mapping (A) demonstrates a slight increase in value in all entire LV walls with subendocardial patterns. Circumferential subendocardial LGE of the anterior, antero-lateral, and infero-lateral LV wall in two-chamber short (B) and of the SIV to the apical segment in long axes (C). Bullseye map of T1 Native (D). LV, left ventricle; LGE, late gadolinium enhancement.
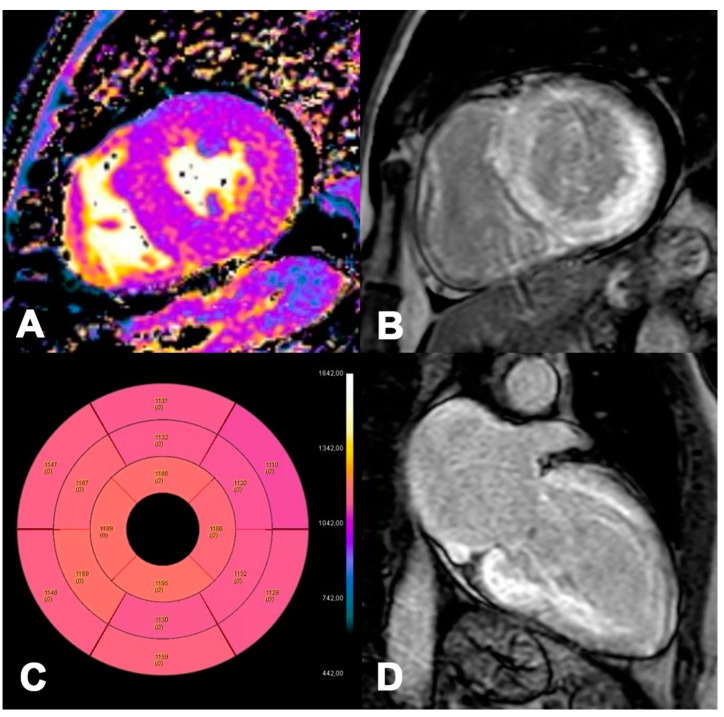
ATTR 73-year-old patient diagnosed with endomyocardial biopsy. T1 Native Mapping (A) demonstrates abnormally high values in all entire LV walls in cardiac amyloidosis. Diffuse transmural LV and subendocardial RV LGE in two-chamber short (B) and long axes (C). Bullseye map of T1 Native (D).
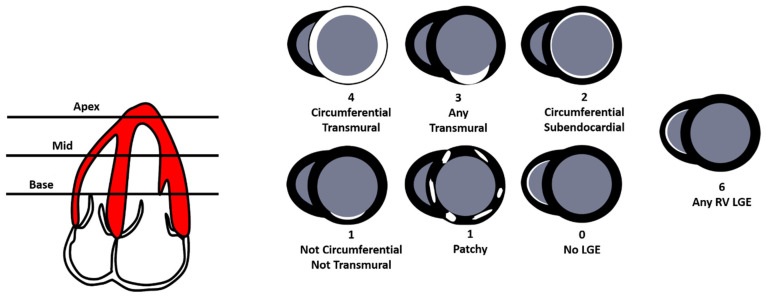
The Query Amyloid Late Enhancement (QALE) score (0–18) is performed on late gadolinium enhancement (LGE) images at the base, mid ventricle, and apex in the left ventricle (LV) and right ventricle (RV). Each LV level is scored according to the degree of LGE, with four points for circumferential and transmural LGE, three points for localized transmural LGE, two points for circumferential subendocardial LGE, one point for localized subendocardial LGE or patchy intramural LGE, and zero points for absent LGE. The maximum LV LGE score level is 12. The presence of any detectable RV LGE scores six.
References
-
- Aimo A., Merlo M., Porcari A., Georgiopoulos G., Pagura L., Vergaro G., Sinagra G., Emdin M., Rapezzi C. Redefining the epidemiology of cardiac amyloidosis. A systematic review and meta-analysis of screening studies. Eur. J. Heart Fail. 2022;24:2342–2351. doi: 10.1002/ejhf.2532. - DOI - PMC - PubMed
-
- Garcia-Pavia P., Rapezzi C., Adler Y., Arad M., Basso C., Brucato A., Burazor I., Caforio A.L.P., Damy T., Eriksson U., et al. Diagnosis and treatment of cardiac amyloidosis. A position statement of the European Society of Cardiology Working Group on myocardial and Pericardial Diseases. Eur. J. Heart Fail. 2021;23:512–526. doi: 10.1002/ejhf.2140. - DOI - PubMed
-
- Dorbala S., Ando Y., Bokhari S., Dispenzieri A., Falk R.H., Ferrari V.A., Fontana M., Gheysens O., Gillmore J.D., Glaudemans A.W.J.M., et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 1 of 2-evidence base and standardized methods of imaging. J. Nucl. Cardiol. 2019;26:2065–2123. doi: 10.1007/s12350-019-01760-6. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
