

Management of Post-Operative Crohn's Disease: Knowns and Unknowns
- PMID: 38673573
- PMCID: PMC11051270
- DOI: 10.3390/jcm13082300
Management of Post-Operative Crohn's Disease: Knowns and Unknowns
Abstract
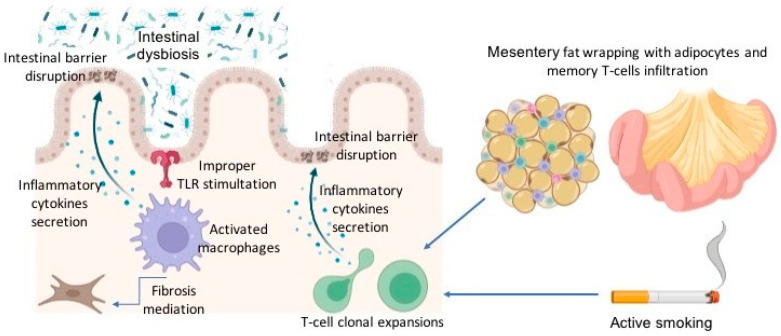
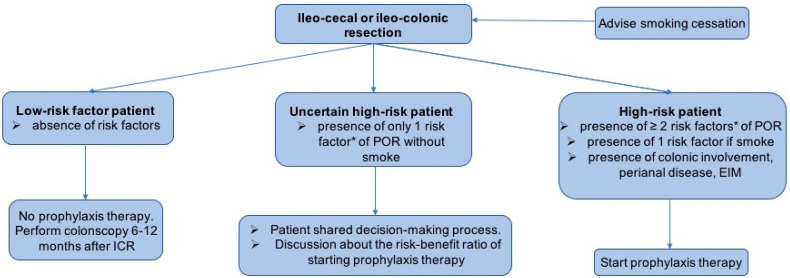
Crohn's disease (CD) is a chronic inflammatory disorder of the gastrointestinal tract characterized by relapsing-remission phases. CD often requires surgical intervention during its course, mainly ileo-cecal/ileo-colonic resection. However, surgery in CD is not curative and post-operative recurrence (POR) can happen. The management of CD after surgery presents challenges. Ensuring timely, effective, and safe therapy to prevent POR is essential but difficult, considering that approximately 20-30% of subjects may not experience endoscopic POR and that 40-50% will only exhibit intermediate lesions, which carry a low risk of mid- and long-term clinical and surgical POR. Currently, there are two accepted intervention strategies: early post-operative prophylactic therapy (systematically or based on the patient's risk of recurrence) or starting therapy after confirming endoscopic POR 6-12 months after surgery (endoscopy-driven prophylactic therapy). The risk of overtreatment lies in exposing patients to undesired adverse events, along with the costs associated with medications. Conversely, undertreatment may lead to missed opportunities to prevent bowel damage and the necessity for additional surgery. This article aims to perform a comprehensive review regarding the optimal strategy to reduce the risk of POR in CD patients and the current therapeutic options.
Keywords: Crohn’s disease; ileo-colonic resection; post-operative recurrence; prophylaxis strategy; risk factors.
Conflict of interest statement
A. Armuzzi has received consulting fees from AbbVie, Allergan, Amgen, Arena, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, MSD, Mylan, Pfizer, Protagonist Therapeutics, Roche, Samsung Bioepis, Sandoz, and Takeda; speaker’s fees from AbbVie, Amgen, Arena, Biogen, Bristol-Myers Squibb, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, MSD, Novartis, Pfizer, Roche, Samsung Bioepis, Sandoz, Takeda, and Tigenix; and research support from Biogen, MSD, Takeda, and Pfizer. C. Bezzio has received lecture fees and served as a consultant for Takeda, MSD, Ferring, Abbvie, Galapagos, Celltrion and Janssen. R. Gabbiadini has received speaker’s fees from Pfizer, Celltrion and MSD. A. Dal Buono has received speaker’s fees from AbbVie, Celltrion and Galapagos. A. Spinelli has received consultation fees from Takeda, Pfizer, Johnson & Johnson, Stryker, and Sofar. A Repici has received consultancy fees from Medtronic, Fuji, Olympus and Erbe; and received research grants and speaker’s fees from Boston Scientific, Erbe, Alfasigma, and Norgine. M. Spertino, A. Busacca, G. Franchellucci and G. Migliorisi declare no conflicts of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
