

Acute Kidney Injury in Patients with Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention: The Role of Vascular Access Site
- PMID: 38673640
- PMCID: PMC11051292
- DOI: 10.3390/jcm13082367
Acute Kidney Injury in Patients with Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention: The Role of Vascular Access Site
Abstract
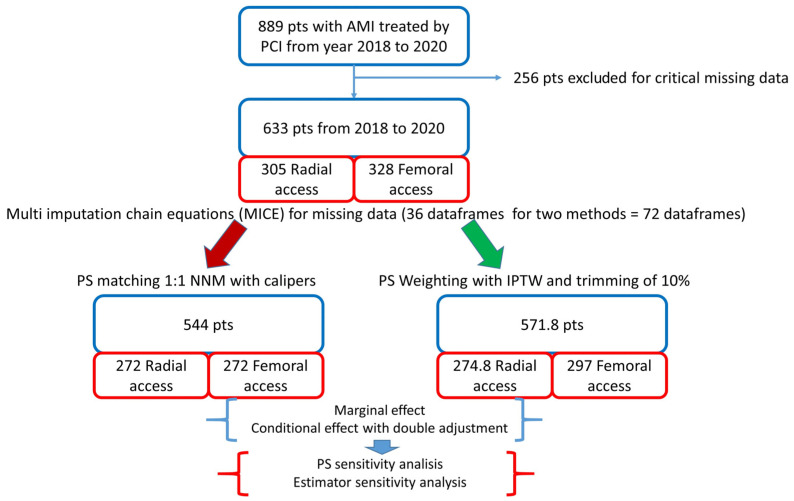
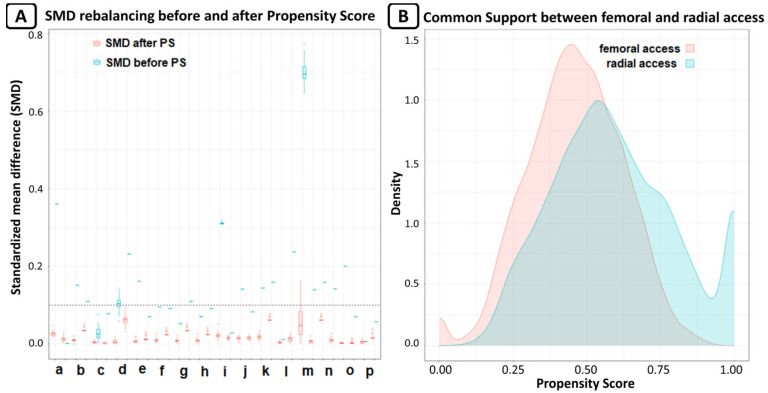
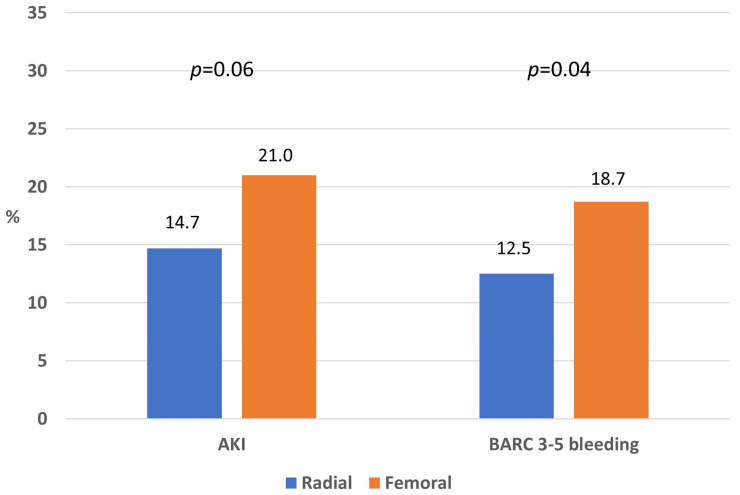
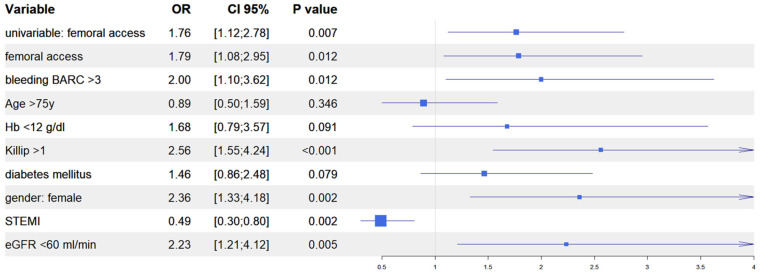
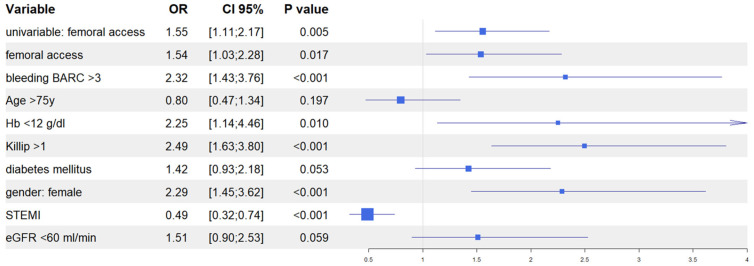
Background: in patients undergoing percutaneous coronary interventions (PCI), radial access should be favoured over femoral access as it reduces the risk of vascular complications and bleeding. Furthermore, a preventive role of radial access in the occurrence of acute kidney injury (AKI), mainly mediated by the reduction of bleeding and cholesterol crystal embolization into renal circulation, has been investigated in several studies, yielding conflicting results. Methods: we designed a retrospective study to appraise the effect of the use of a vascular access site on the occurrence of AKI in a cohort of 633 patients with acute myocardial infarction treated by PCI at our centre from 2018 to 2020. Results: after propensity score adjustment, radial access was associated with a reduced, albeit statistically not significant, incidence of AKI (14.7% vs. 21.0%; p = 0.06) and major bleeding (12.5% vs. 18.7%; p = 0.04) as compared to femoral access. At multivariate analysis, femoral access was an independent predictor of AKI, together with in-hospital occurrence of BARC 3-5 bleeding, Killip class >1 at presentation, female gender, baseline eGFR <60 mL/min, and baseline haemoglobin <12 g/dL. Conclusions: although limited by the observational design, our study supports the hypothesis that radial access may exert a protective role on the occurrence of AKI in patients with acute myocardial infarction undergoing PCI.
Keywords: NSTEMI; STEMI; multivessel disease.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Giacoppo D., Madhavan M.V., Baber U., Warren J., Bansilal S., Witzenbichler B., Dangas G.D., Kirtane A.J., Xu K., Kornowski R., et al. Impact of Contrast-Induced Acute Kidney Injury after Percutaneous Coronary Intervention on Short- and Long-Term Outcomes: Pooled Analysis from the HORIZONS-AMI and ACUITY Trials. Circ. Cardiovasc. Interv. 2015;8:e002475. doi: 10.1161/CIRCINTERVENTIONS.114.002475. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
