

Exploring Advanced Therapies for Primary Biliary Cholangitis: Insights from the Gut Microbiota-Bile Acid-Immunity Network
- PMID: 38673905
- PMCID: PMC11050225
- DOI: 10.3390/ijms25084321
Exploring Advanced Therapies for Primary Biliary Cholangitis: Insights from the Gut Microbiota-Bile Acid-Immunity Network
Abstract
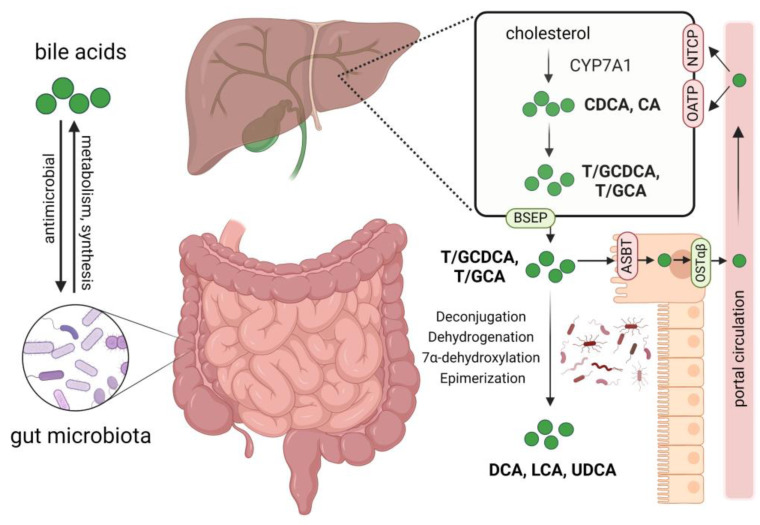
Primary biliary cholangitis (PBC) is a cholestatic liver disease characterized by immune-mediated injury to small bile ducts. Although PBC is an autoimmune disease, the effectiveness of conventional immunosuppressive therapy is disappointing. Nearly 40% of PBC patients do not respond to the first-line drug UDCA. Without appropriate intervention, PBC patients eventually progress to liver cirrhosis and even death. There is an urgent need to develop new therapies. The gut-liver axis emphasizes the interconnection between the gut and the liver, and evidence is increasing that gut microbiota and bile acids play an important role in the pathogenesis of cholestatic diseases. Dysbiosis of gut microbiota, imbalance of bile acids, and immune-mediated bile duct injury constitute the triad of pathophysiology in PBC. Autoimmune cholangitis has the potential to be improved through immune system modulation. Considering the failure of conventional immunotherapies and the involvement of gut microbiota and bile acids in the pathogenesis, targeting immune factors associated with them, such as bile acid receptors, microbial-derived molecules, and related specific immune cells, may offer breakthroughs. Understanding the gut microbiota-bile acid network and related immune dysfunctions in PBC provides a new perspective on therapeutic strategies. Therefore, we summarize the latest advances in research of gut microbiota and bile acids in PBC and, for the first time, explore the possibility of related immune factors as novel immunotherapy targets. This article discusses potential therapeutic approaches focusing on regulating gut microbiota, maintaining bile acid homeostasis, their interactions, and related immune factors.
Keywords: bile acid; gut microbiota; primary biliary cholangitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Bile acids and intestinal microbiota in autoimmune cholestatic liver diseases.Autoimmun Rev. 2017 Sep;16(9):885-896. doi: 10.1016/j.autrev.2017.07.002. Epub 2017 Jul 8. Autoimmun Rev. 2017. PMID: 28698093 Review.
-
Comprehensive Analysis of Serum and Fecal Bile Acid Profiles and Interaction with Gut Microbiota in Primary Biliary Cholangitis.Clin Rev Allergy Immunol. 2020 Feb;58(1):25-38. doi: 10.1007/s12016-019-08731-2. Clin Rev Allergy Immunol. 2020. PMID: 30900136
-
The gut microbial influence on cholestatic liver disease.Liver Int. 2019 Jul;39(7):1186-1196. doi: 10.1111/liv.14153. Epub 2019 Jun 17. Liver Int. 2019. PMID: 31125502 Review.
-
The fecal microbiota of patients with primary biliary cholangitis (PBC) causes PBC-like liver lesions in mice and exacerbates liver damage in a mouse model of PBC.Gut Microbes. 2024 Jan-Dec;16(1):2383353. doi: 10.1080/19490976.2024.2383353. Epub 2024 Aug 6. Gut Microbes. 2024. PMID: 39105259 Free PMC article.
-
PPAR-Mediated Bile Acid Glucuronidation: Therapeutic Targets for the Treatment of Cholestatic Liver Diseases.Cells. 2024 Aug 1;13(15):1296. doi: 10.3390/cells13151296. Cells. 2024. PMID: 39120326 Free PMC article. Review.
Cited by
-
Bibliometric analysis of research on intestinal flora and primary biliary cholangitis published between 2004 and 2024 using VOSviewer and CiteSpace visualization.Front Med (Lausanne). 2025 May 21;12:1565778. doi: 10.3389/fmed.2025.1565778. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40470048 Free PMC article.
-
Breaking Grounds: A Comprehensive Analysis of Cutting-Edge Treatments for Primary Biliary Cirrhosis/Primary Biliary Cholangitis With Futuristic Treatments.Cureus. 2025 Feb 24;17(2):e79582. doi: 10.7759/cureus.79582. eCollection 2025 Feb. Cureus. 2025. PMID: 40151700 Free PMC article. Review.
-
Primary biliary cholangitis: a summary of pathogenesis and therapies.Ann Gastroenterol. 2025 Mar-Apr;38(2):121-132. doi: 10.20524/aog.2025.0953. Epub 2025 Feb 28. Ann Gastroenterol. 2025. PMID: 40124425 Free PMC article. Review.
-
Metallothioneins in the Pathogenesis of Liver Diseases: A Review.Int J Hepatol. 2025 Jul 25;2025:8880889. doi: 10.1155/ijh/8880889. eCollection 2025. Int J Hepatol. 2025. PMID: 40755507 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
