

The Effect of Intraoperative Patient Positioning on the Success of Intertrochanteric Fracture Surgery in Older Patients
- PMID: 38674292
- PMCID: PMC11052214
- DOI: 10.3390/medicina60040646
The Effect of Intraoperative Patient Positioning on the Success of Intertrochanteric Fracture Surgery in Older Patients
Abstract
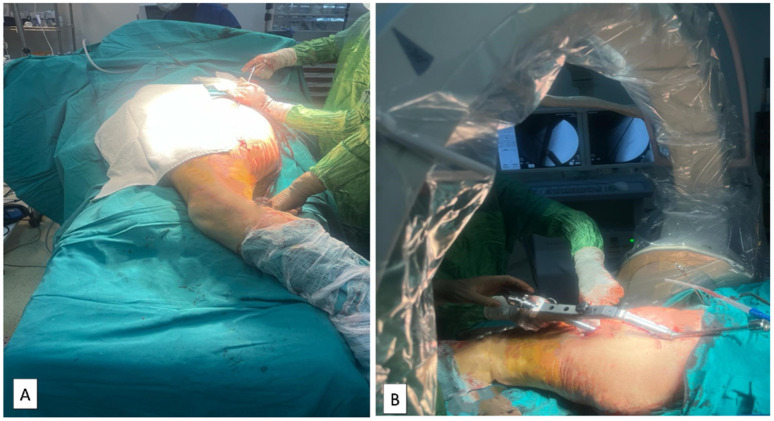
Background and Objectives: The incidence of hip fractures in people of advanced ages is increasing due to our aging society. Patient positioning for the intertrochanteric fractures of the femur can be performed in various ways. The aim of this study is to clinically and radiologically compare the use of the supine hemilithotomy position, the lateral decubitus position, and the traction table when performing proximal femoral nail (PFN) surgery for femoral intertrochanteric fractures in the geriatric age group. Materials and Methods: A total of 170 elderly patients with femoral intertrochanteric fractures were included in this cross-sectional study. The patients were divided into three groups (the supine hemilithotomy group, the lateral decubitus group, and the fracture table group). For the postoperative period, complications, length of stay in the intensive care unit, and length of stay in hospital were examined, while in postoperative radiographs, tip-apex distances (TADs), collodiaphyseal angles (CDAs), and Cleveland-Bosworth quadrants were examined to evaluate the placement of the lag screw in the femoral head. The quality of fracture reduction was evaluated according to the modified Baumgaertner criteria. Results: The mean age of the patients was 77.8 ± 8.8; 57.6% of patients were female. According to the modified Baumgaertner criteria, it was determined that patients with 'poor' reduction quality had an approximately ten times higher risk of cut-out than those with 'good' reduction quality (OR = 10.111, p = 0.002, 95% confidence interval; 2.313-44.207). The operative time for patients in the fracture table group was longer than that of the other groups Additionally, the CDA in the supine hemilithotomy position group was longer. Conclusions: Although PFN surgery using the traction table is longer in terms of surgical time compared to surgery performed in the lateral decubitus position and the supine hemilitotomy position, it is advantageous in terms of better TAD and CDA values and lower complication rates.
Keywords: PFN; intertrochanteric fracture; lateral decubitus; supine hemilithotomy; traction table.
Conflict of interest statement
There are no conflicts of interest to declare.
Figures





References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
