

Noninvasive Ambulatory Electrocardiographic Markers from Patients with COVID-19 Pneumonia: A Report of Three Cases
- PMID: 38674301
- PMCID: PMC11052239
- DOI: 10.3390/medicina60040655
Noninvasive Ambulatory Electrocardiographic Markers from Patients with COVID-19 Pneumonia: A Report of Three Cases
Abstract
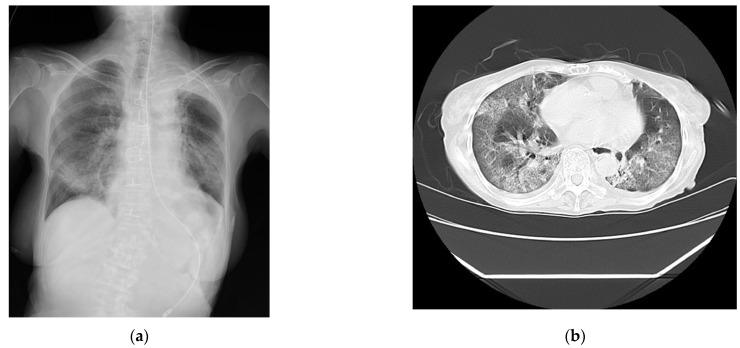
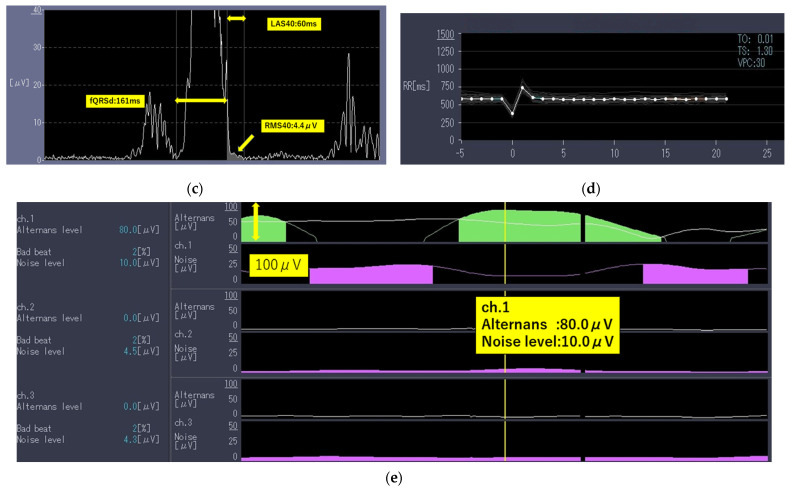
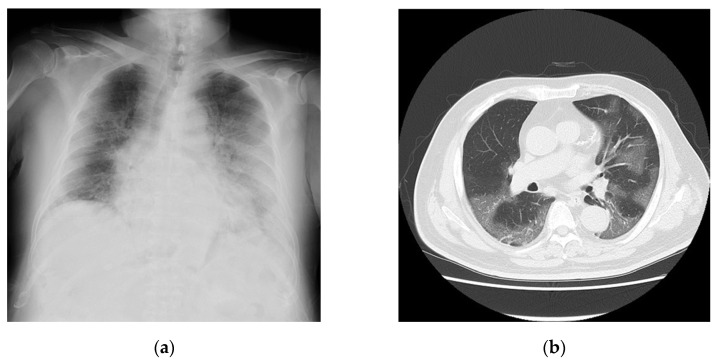
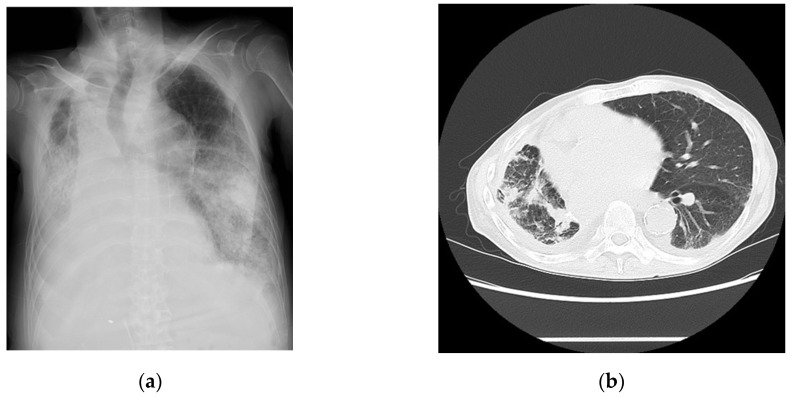
Coronavirus disease 2019 (COVID-19) has affected medical practice. More than 7,000,000 patients died worldwide after being infected with COVID-19; however, no specific laboratory markers have yet been established to predict death related to this disease. In contrast, electrocardiographic changes due to COVID-19 include QT prolongation and ST-T changes; however, there have not been studies on the ambulatory electrocardiographic markers of COVID-19. We encountered three patients diagnosed as having COVID-19 who did not have a prior history of significant structural heart diseases. All patients had abnormalities in ambulatory echocardiogram parameters detected by high-resolution 24 h electrocardiogram monitoring: positive late potentials (LPs) and T-wave alternans (TWA), abnormal heart rate variability (HRV), and heart rate turbulence (HRT). Case 1 involved a 78-year-old woman with a history of chronic kidney disease, Case 2 involved a 76-year-old man with hypertension and diabetes, and Case 3 involved a 67-year-old man with renal cancer, lung cancer, and diabetes. None of them had a prior history of significant structural heart disease. Although no significant consistent increases in clinical markers were observed, all three patients died, mainly because of respiratory failure with mild heart failure. The LP, TWA, HRV, and HRT were positive in all three cases with no significant structural cardiac disease at the initial phase of admission. The further accumulation of data regarding ambulatory electrocardiographic markers in patients with COVID-19 is needed. Depending on the accumulation of data, the LP, TWA, HRV, and HRT could be identified as potential risk factors for COVID-19 pneumonia in the early phase of admission.
Keywords: COVID-19; Holter electrocardiograph; SARS-CoV-2; ambulatory electrocardiographic markers; coronavirus disease-19; global cardiac ischemia; myocardial remodeling; sudden cardiac death.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- World Health Organization Number of COVID-19 deaths reported to WHO. [(accessed on 21 February 2024)]. Available online: https://data.who.int/dashboards/covid19/deaths?n=c.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
