

Principles in the Management of Glioblastoma
- PMID: 38674436
- PMCID: PMC11050118
- DOI: 10.3390/genes15040501
Principles in the Management of Glioblastoma
Abstract
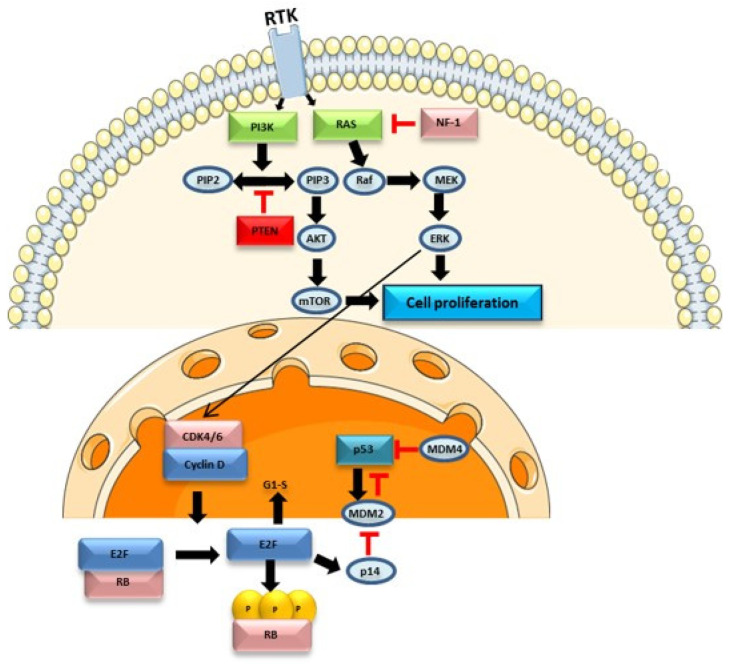
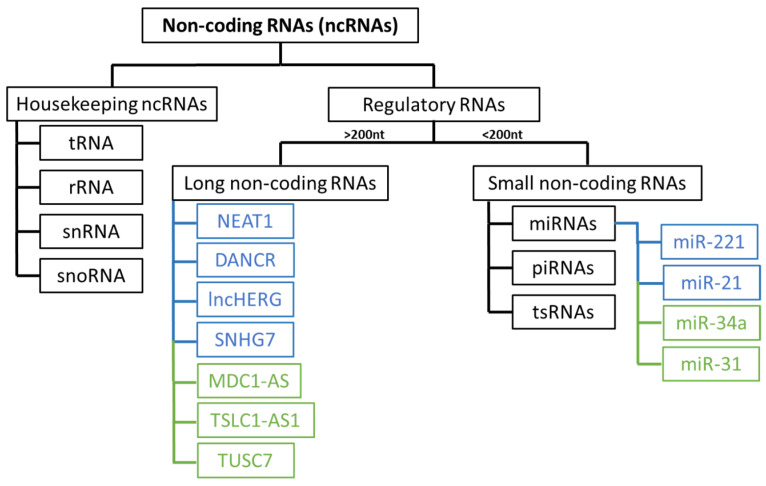
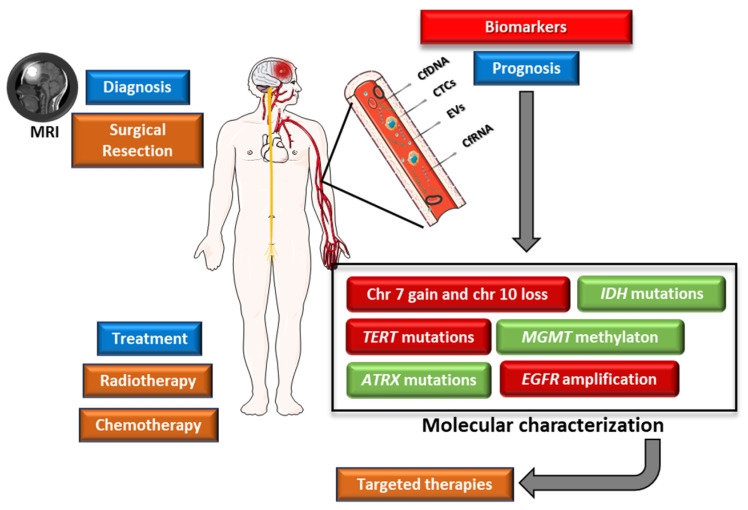
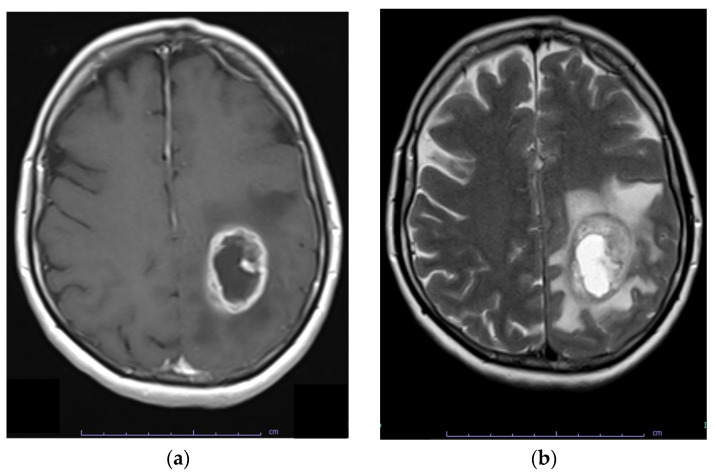
Glioblastoma, the most aggressive and common malignant primary brain tumour, is characterized by infiltrative growth, abundant vascularization, and aggressive clinical evolution. Patients with glioblastoma often face poor prognoses, with a median survival of approximately 15 months. Technological progress and the subsequent improvement in understanding the pathophysiology of these tumours have not translated into significant achievements in therapies or survival outcomes for patients. Progress in molecular profiling has yielded new omics data for a more refined classification of glioblastoma. Several typical genetic and epigenetic alterations in glioblastoma include mutations in genes regulating receptor tyrosine kinase (RTK)/rat sarcoma (RAS)/phosphoinositide 3-kinase (PI3K), p53, and retinoblastoma protein (RB) signalling, as well as mutation of isocitrate dehydrogenase (IDH), methylation of O6-methylguanine-DNA methyltransferase (MGMT), amplification of epidermal growth factor receptor vIII, and codeletion of 1p/19q. Certain microRNAs, such as miR-10b and miR-21, have also been identified as prognostic biomarkers. Effective treatment options for glioblastoma are limited. Surgery, radiotherapy, and alkylating agent chemotherapy remain the primary pillars of treatment. Only promoter methylation of the gene MGMT predicts the benefit from alkylating chemotherapy with temozolomide and it guides the choice of first-line treatment in elderly patients. Several targeted strategies based on tumour-intrinsic dominant signalling pathways and antigenic tumour profiles are under investigation in clinical trials. This review explores the potential genetic and epigenetic biomarkers that could be deployed as analytical tools in the diagnosis and prognostication of glioblastoma. Recent clinical advancements in treating glioblastoma are also discussed, along with the potential of liquid biopsies to advance personalized medicine in the field of glioblastoma, highlighting the challenges and promises for the future.
Keywords: genetic and epigenetic biomarkers; glioblastoma; liquid biopsies; mutations; signaling pathways; target therapies.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Perry A., Wesseling P. Handbook of Clinical Neurology. Elsevier; Amsterdam, The Netherlands: 2016. Histologic Classification of Gliomas; pp. 71–95. - PubMed
-
- Tamimi A.F., Juweid M. Glioblastoma. Codon Publications; Singapore: 2017. Epidemiology and Outcome of Glioblastoma; pp. 143–153. - PubMed
-
- Wang Q., Hu B., Hu X., Kim H., Squatrito M., Scarpace L., de Carvalho A.C., Lyu S., Li P., Li Y., et al. Tumor Evolution of Glioma-Intrinsic Gene Expression Subtypes Associates with Immunological Changes in the Microenvironment. Cancer Cell. 2017;32:42–56.e6. doi: 10.1016/j.ccell.2017.06.003. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
