

Severe Tick-Borne Encephalitis (TBE) in a Patient with X-Linked Agammaglobulinemia; Treatment with TBE Virus IgG Positive Plasma, Clinical Outcome and T Cell Responses
- PMID: 38676861
- PMCID: PMC11055791
- DOI: 10.1007/s10875-024-01718-5
Severe Tick-Borne Encephalitis (TBE) in a Patient with X-Linked Agammaglobulinemia; Treatment with TBE Virus IgG Positive Plasma, Clinical Outcome and T Cell Responses
Abstract
Purpose: A patient with X-linked agammaglobulinemia (XLA) and severe tick-borne encephalitis (TBE) was treated with TBE virus (TBEV) IgG positive plasma. The patient's clinical response, humoral and cellular immune responses were characterized pre- and post-infection.
Methods: ELISA and neutralisation assays were performed on sera and TBEV PCR assay on sera and cerebrospinal fluid. T cell assays were conducted on peripheral blood the patient and five healthy vaccinated controls.
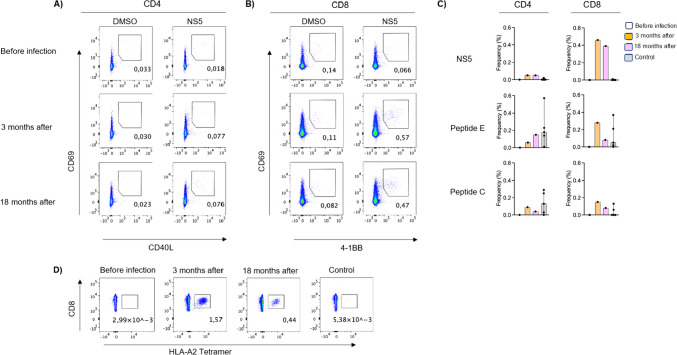
Results: The patient was admitted to the hospital with headache and fever. He was not vaccinated against TBE but receiving subcutaneous IgG-replacement therapy (IGRT). TBEV IgG antibodies were low-level positive (due to scIGRT), but the TBEV IgM and TBEV neutralisation tests were negative. During hospitalisation his clinical condition deteriorated (Glasgow coma scale 3/15) and he was treated in the ICU with corticosteroids and external ventricular drainage. He was then treated with plasma containing TBEV IgG without apparent side effects. His symptoms improved within a few days and the TBEV neutralisation test converted to positive. Robust CD8+ T cell responses were observed at three and 18-months post-infection, in the absence of B cells. This was confirmed by tetramers specific for TBEV.
Conclusion: TBEV IgG-positive plasma given to an XLA patient with TBE without evident adverse reactions may have contributed to a positive clinical outcome. Similar approaches could offer a promising foundation for researching therapeutic options for patients with humoral immunodeficiencies. Importantly, a robust CD8+ T cell response was observed after infection despite the lack of B cells and indicates that these patients can clear acute viral infections and could benefit from future vaccination programs.
Keywords: CD8+ T cells; X-linked agammaglobulinemia; immunodeficiency; neutralising antibodies; tetramers; tick-borne encephalitis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Kinetics of tick-borne encephalitis virus IgM antibody responses in serum and cerebrospinal fluid.Infect Dis (Lond). 2025 Jul;57(7):676-686. doi: 10.1080/23744235.2025.2473496. Epub 2025 Mar 24. Infect Dis (Lond). 2025. PMID: 40126069
-
A Retrospective Sero-Surveillance Study for Antibodies Against Tick-Borne Encephalitis Virus in Norway.Viruses. 2025 Feb 20;17(3):291. doi: 10.3390/v17030291. Viruses. 2025. PMID: 40143223 Free PMC article.
-
Immunogenicity against Far Eastern and Siberian subtypes of tick-borne encephalitis (TBE) virus elicited by the currently available vaccines based on the European subtype: systematic review and meta-analysis.Hum Vaccin Immunother. 2014;10(10):2819-33. doi: 10.4161/hv.29984. Hum Vaccin Immunother. 2014. PMID: 25483679 Free PMC article.
-
Incidence of tick-borne encephalitis (TBE) in the pediatric population at the University Hospitals of Strasbourg (HUS) and characterization of confirmed cases.J Neurovirol. 2024 Dec;30(5-6):534-544. doi: 10.1007/s13365-024-01233-8. Epub 2024 Oct 31. J Neurovirol. 2024. PMID: 39480620
-
Clinical manifestations and outcomes of Tick-borne encephalitis: A systematic literature review.Ticks Tick Borne Dis. 2024 Nov;15(6):102407. doi: 10.1016/j.ttbdis.2024.102407. Epub 2024 Nov 4. Ticks Tick Borne Dis. 2024. PMID: 39500220
Cited by
-
Tick-Borne Encephalitis Virus Infection in a Two-Year-Old Child Returning from Switzerland (July-August 2023): Is It Time for TBE Immunization of Serbian Travelers?Pathogens. 2024 Nov 18;13(11):1013. doi: 10.3390/pathogens13111013. Pathogens. 2024. PMID: 39599566 Free PMC article.
-
An autochthonous case of severe tick-borne encephalitis virus associated meningoencephalitis in France: Is there a place for polyvalent intravenous immunoglobulins?IDCases. 2025 Mar 31;40:e02213. doi: 10.1016/j.idcr.2025.e02213. eCollection 2025. IDCases. 2025. PMID: 40237002 Free PMC article.
-
Dysregulation of Toll-Like Receptor Signaling-Associated Gene Expression in X-Linked Agammaglobulinemia: Implications for Correlations Genotype-Phenotype and Disease Expression.J Innate Immun. 2024;16(1):425-439. doi: 10.1159/000540082. Epub 2024 Aug 8. J Innate Immun. 2024. PMID: 39116841 Free PMC article.
References
-
- Schaafsma GC, Väliaho J, Wang Q, Berglöf A, Zain R, Smith CI, Vihinen M. BTKbase, Bruton Tyrosine Kinase Variant Database in X-Linked Agammaglobulinemia: Looking Back and Ahead. Human Mutation. 2023;1–12:2023. doi: 10.1155/2023/5797541. - DOI
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
