

Rapid Diagnostic Tests and Antimicrobial Stewardship Programs for the Management of Bloodstream Infection: What Is Their Relative Contribution to Improving Clinical Outcomes? A Systematic Review and Network Meta-analysis
- PMID: 38676943
- PMCID: PMC11327801
- DOI: 10.1093/cid/ciae234
Rapid Diagnostic Tests and Antimicrobial Stewardship Programs for the Management of Bloodstream Infection: What Is Their Relative Contribution to Improving Clinical Outcomes? A Systematic Review and Network Meta-analysis
Abstract
Background: Evidence about the clinical impact of rapid diagnostic tests (RDTs) for the diagnosis of bloodstream infections is limited, and whether RDT are superior to conventional blood cultures (BCs) embedded within antimicrobial stewardship programs (ASPs) is unknown.
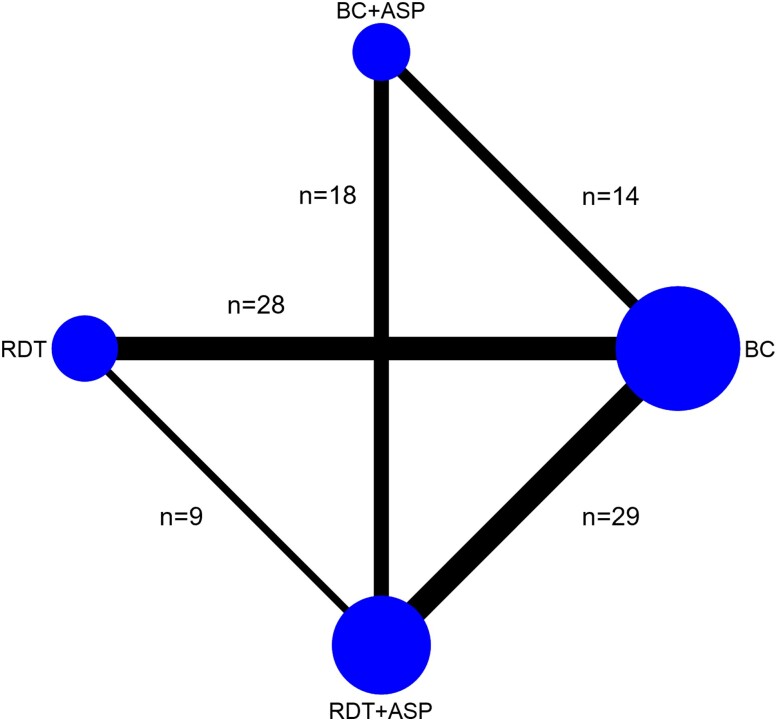
Methods: We performed network meta-analyses using results from studies of patients with bloodstream infection with the aim of comparing the clinical impact of RDT (applied on positive BC broth or whole blood) to conventional BC, both assessed with and without ASP with respect to mortality, length of stay (LOS), and time to optimal therapy.
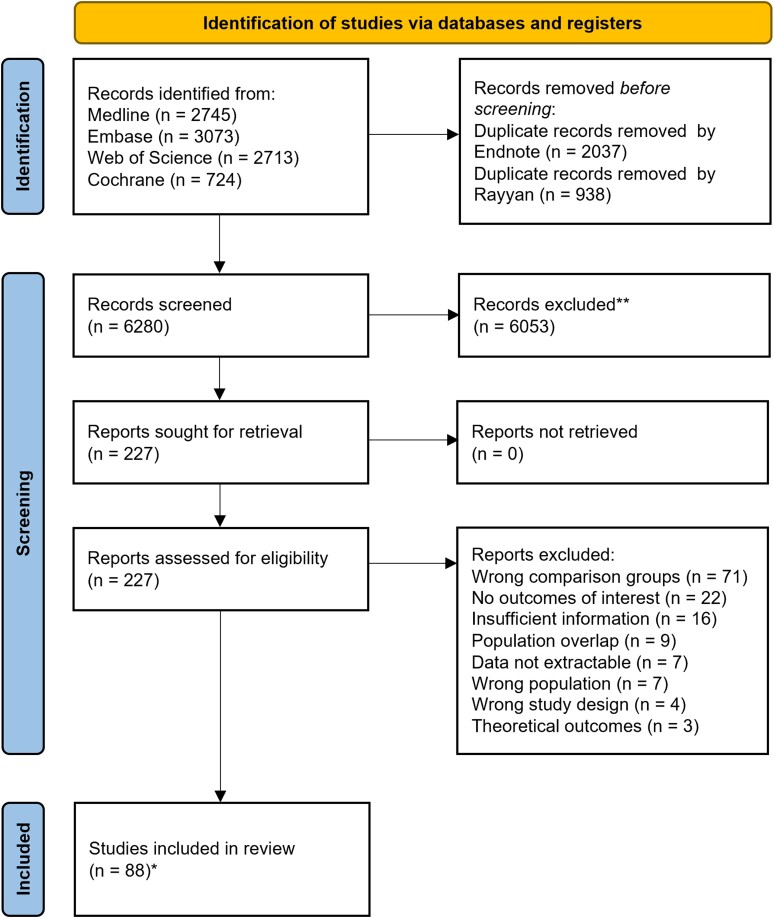
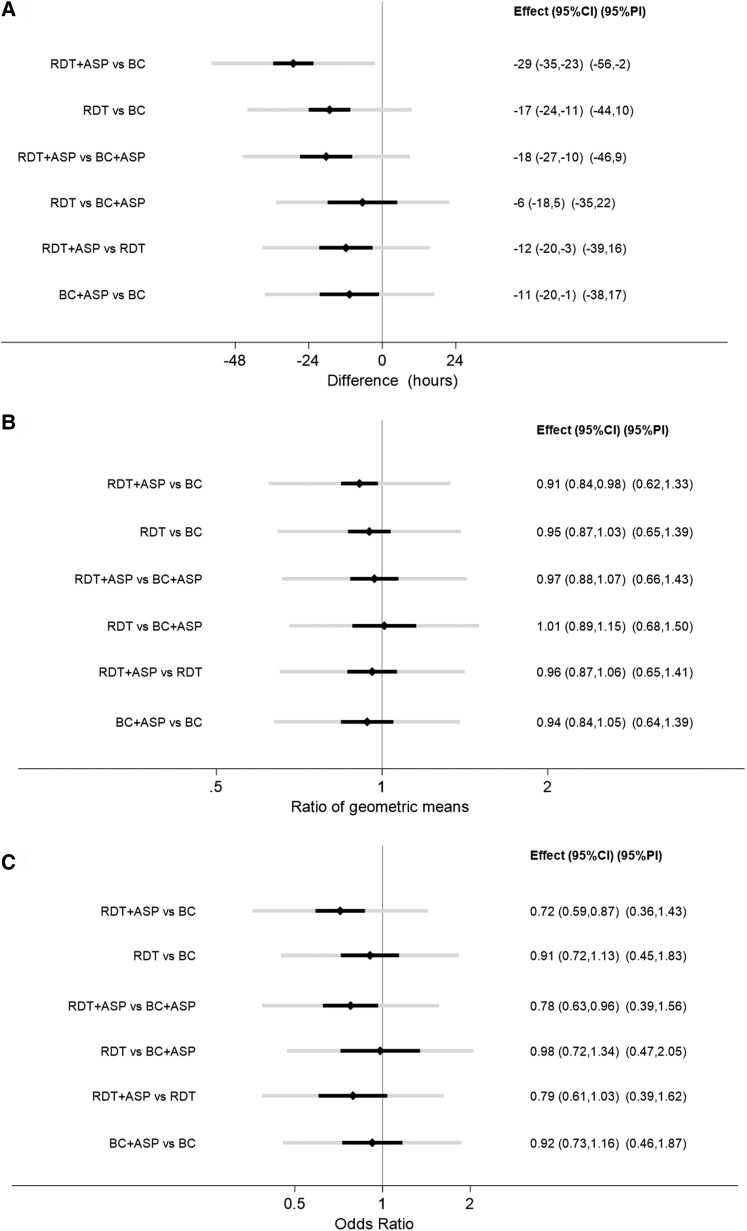
Results: Eighty-eight papers were selected, including 25 682 patient encounters. There was an appreciable amount of statistical heterogeneity within each meta-analysis. The network meta-analyses showed a significant reduction in mortality associated with the use of RDT + ASP versus BC alone (odds ratio [OR], 0.72; 95% confidence interval [CI], .59-.87) and with the use of RDT + ASP versus BC + ASP (OR, 0.78; 95% CI, .63-.96). No benefit in survival was found associated with the use of RDT alone nor with BC + ASP compared to BC alone. A reduction in LOS was associated with RDT + ASP versus BC alone (OR, 0.91; 95% CI, .84-.98) whereas no difference in LOS was shown between any other groups. A reduced time to optimal therapy was shown when RDT + ASP was compared to BC alone (-29 hours; 95% CI, -35 to -23), BC + ASP (-18 hours; 95% CI, -27 to -10), and to RDT alone (-12 hours; 95% CI, -20 to -3).
Conclusions: The use of RDT + ASP may lead to a survival benefit even when introduced in settings already adopting effective ASP in association with conventional BC.
Keywords: antimicrobial stewardship; blood culture; bloodstream infection; network meta-analysis; rapid diagnostic tests.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest . D. L. P. has research funding from Shionogi, Merck, bioMerieux, BioVersys, and Pfizer and has received consulting fees from the AMR Action Fund, CARB-X, Aurobac, Pfizer, Merck, Cepheid, bioMérieux, and Spero. P. N. A. H. reports research grants from Gilead, has served on advisory boards for OpGen, Merck, and Sandoz, and has received honoraria from OpGen, Sandoz, Pfizer, and bioMerieux. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med 2014; 42:1749–55. - PubMed
-
- Sweeney TE, Liesenfeld O, May L. Diagnosis of bacterial sepsis: why are tests for bacteremia not sufficient? Expert Rev Mol Diagn 2019; 19:959–62. - PubMed
-
- Lamy B, Sundqvist M, Idelevich EA; ESCMID Study Group for Bloodstream Infections, Endocarditis and Sepsis (ESGBIES) . Bloodstream infections—standard and progress in pathogen diagnostics. Clin Microbiol Infect 2020; 26: 142–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
