

Temporal changes in SARS-CoV-2 clearance kinetics and the optimal design of antiviral pharmacodynamic studies: an individual patient data meta-analysis of a randomised, controlled, adaptive platform study (PLATCOV)
- PMID: 38677300
- PMCID: PMC7617756
- DOI: 10.1016/S1473-3099(24)00183-X
Temporal changes in SARS-CoV-2 clearance kinetics and the optimal design of antiviral pharmacodynamic studies: an individual patient data meta-analysis of a randomised, controlled, adaptive platform study (PLATCOV)
Abstract
Background: Effective antiviral drugs prevent hospitalisation and death from COVID-19. Antiviral efficacy can be efficiently assessed in vivo by measuring rates of SARS-CoV-2 clearance estimated from serial viral genome densities quantitated in nasopharyngeal or oropharyngeal swab eluates. We conducted an individual patient data meta-analysis of unblinded arms in the PLATCOV platform trial to characterise changes in viral clearance kinetics and infer optimal design and interpretation of antiviral pharmacometric evaluations.
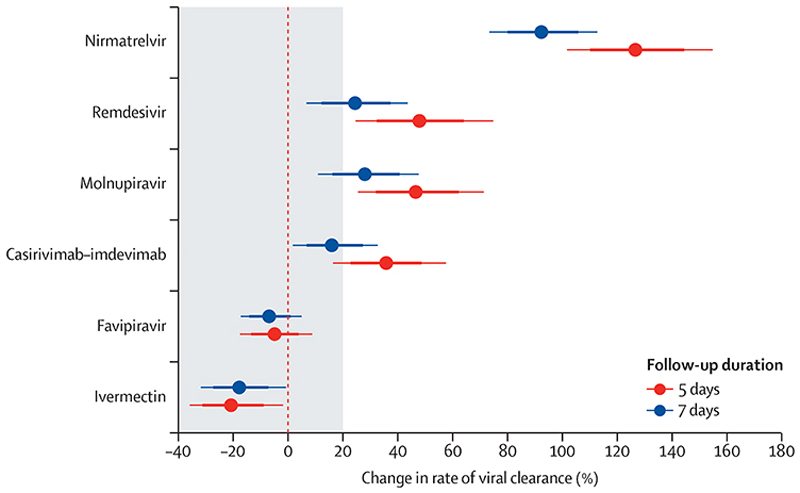
Methods: Serial viral density data were analysed from symptomatic, previously healthy, adult patients (within 4 days of symptom onset) enrolled in a large multicentre, randomised, adaptive, pharmacodynamic, platform trial (PLATCOV) comparing antiviral interventions for SARS-CoV-2. Viral clearance rates over 1 week were estimated under a hierarchical Bayesian linear model with B-splines used to characterise temporal changes in enrolment viral densities and clearance rates. Bootstrap re-sampling was used to assess the optimal duration of follow-up for pharmacometric assessment, where optimal was defined as maximising the expected Z score when comparing effective antivirals with no treatment. PLATCOV is registered at ClinicalTrials.gov, NCT05041907.
Findings: Between Sept 29, 2021, and Oct 20, 2023, 1262 patients were randomly assigned in the PLATCOV trial. Unblinded data were available from 800 patients (who provided 16 818 oropharyngeal viral quantitative PCR [qPCR] measurements), of whom 504 (63%) were female. 783 (98%) patients had received at least one vaccine dose and 703 (88%) were fully vaccinated. SARS-CoV-2 viral clearance was biphasic (bi-exponential). The first phase (α) was accelerated by effective interventions. For all the effective interventions studied, maximum discriminative power (maximum expected Z score) was obtained when evaluating serial data from the first 5 days after enrolment. Over the 2-year period studied, median viral clearance half-lives estimated over 7 days shortened from 16·6 h (IQR 15·3 to 18·2) in September, 2021, to 9·2 h (8·0 to 10·6) in October, 2023, in patients receiving no antiviral drugs, equivalent to a relative reduction of 44% (95% credible interval [CrI] 19 to 64). A parallel reduction in viral clearance half-lives over time was observed in patients receiving antiviral drugs. For example, in the 158 patients assigned to ritonavir-boosted nirmatrelvir (3380 qPCR measurements), the median viral clearance half-life reduced from 6·4 h (IQR 5·7 to 7·3) in June, 2022, to 4·8 h (4·2 to 5·5) in October, 2023, a relative reduction of 26% (95% CrI -4 to 42).
Interpretation: SARS-CoV-2 viral clearance kinetics in symptomatic, vaccinated individuals accelerated substantially over 2 years of the pandemic, necessitating a change to how new SARS-CoV-2 antivirals are compared (ie, shortening the period of pharmacodynamic assessment). As of writing (October, 2023), antiviral efficacy in COVID-19 can be efficiently assessed in vivo using serial qPCRs from duplicate oropharyngeal swab eluates taken daily for 5 days after drug administration.
Funding: Wellcome Trust.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures




References
-
- Schilling WHK, Jittamala P, Watson JA, et al. Antiviral efficacy of molnupiravir versus ritonavir-boosted nirmatrelvir in patients with early symptomatic COVID-19 (PLATCOV): an open-label, phase 2, randomised, controlled, adaptive trial. Lancet Infect Dis. 2024;24:36–45. doi: 10.1016/S1473-3099(23)00493-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
