

Interferon-gamma signature as prognostic and predictive marker in macroscopic stage III melanoma
- PMID: 38677880
- PMCID: PMC11057279
- DOI: 10.1136/jitc-2023-008125
Interferon-gamma signature as prognostic and predictive marker in macroscopic stage III melanoma
Abstract
Background: A substantial proportion of patients with macroscopic stage III melanoma do not benefit sufficiently from adjuvant anti-PD-1 therapy, as they either recur despite therapy or would never have recurred. To better inform adjuvant treatment selection, we have performed translational analyses to identify prognostic and predictive biomarkers.
Patients and methods: Two cohorts of patients with macroscopic stage III melanoma from an ongoing biobank study were included. Clinical data were compared between an observation cohort (cohort 1) and an adjuvant intention cohort (cohort 2). RNA sequencing for translational analyses was performed and treatment subgroups (cohort 1A and cohort 2A) were compared for possible biomarkers, using a cut-off based on the treatment-naïve patients. In addition, two validation cohorts (Melanoma Institute Australia (MIA) and University Medical Centre Utrecht (UMCU)) were obtained.
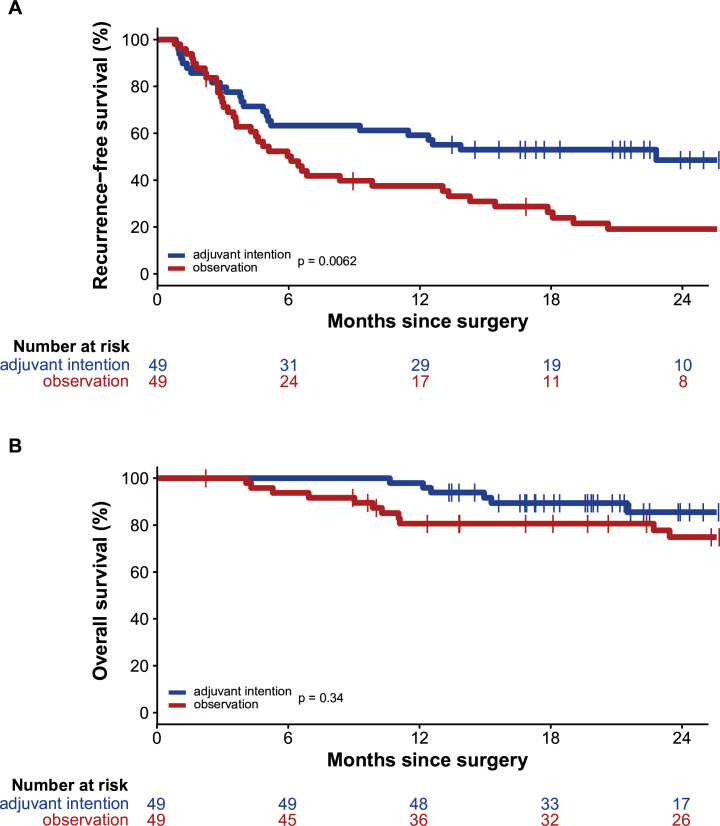
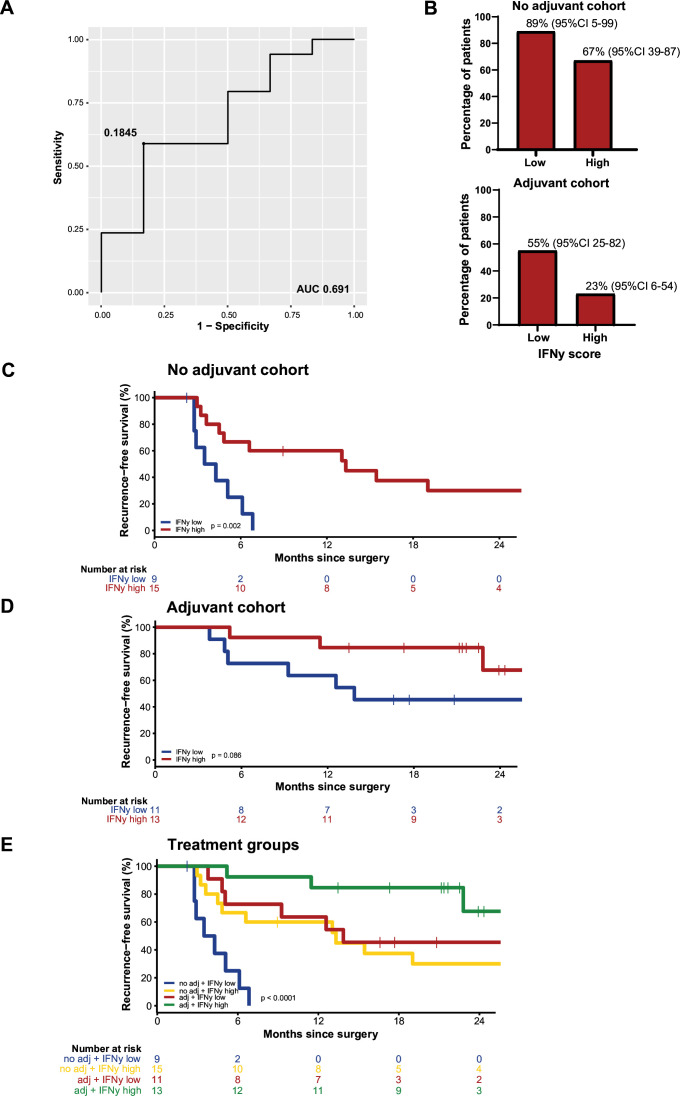
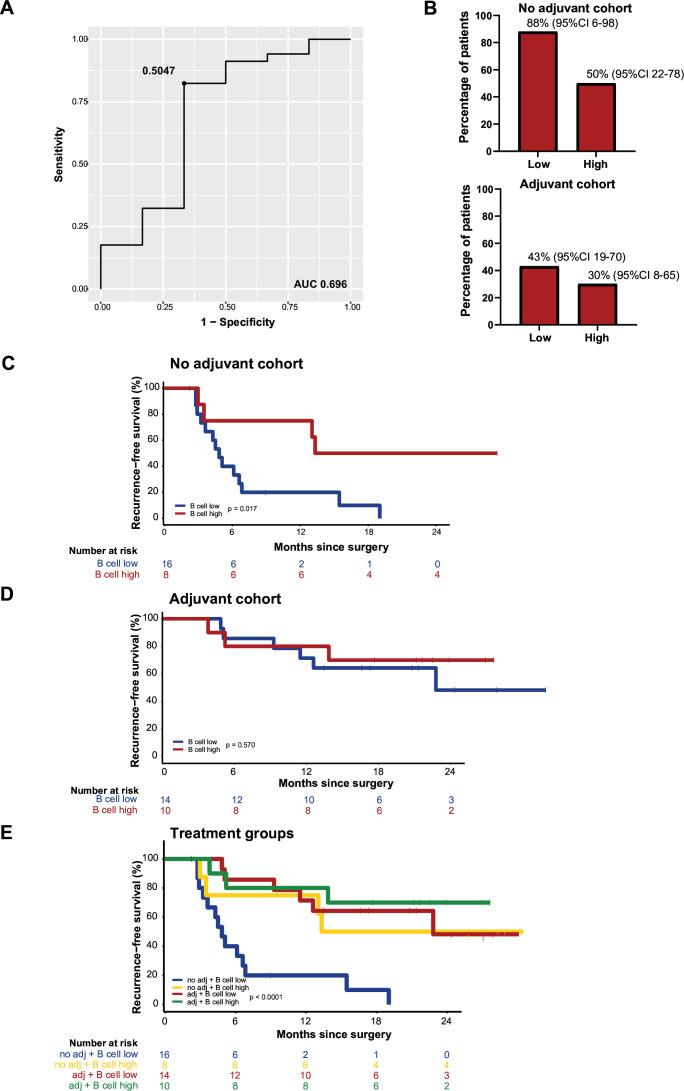
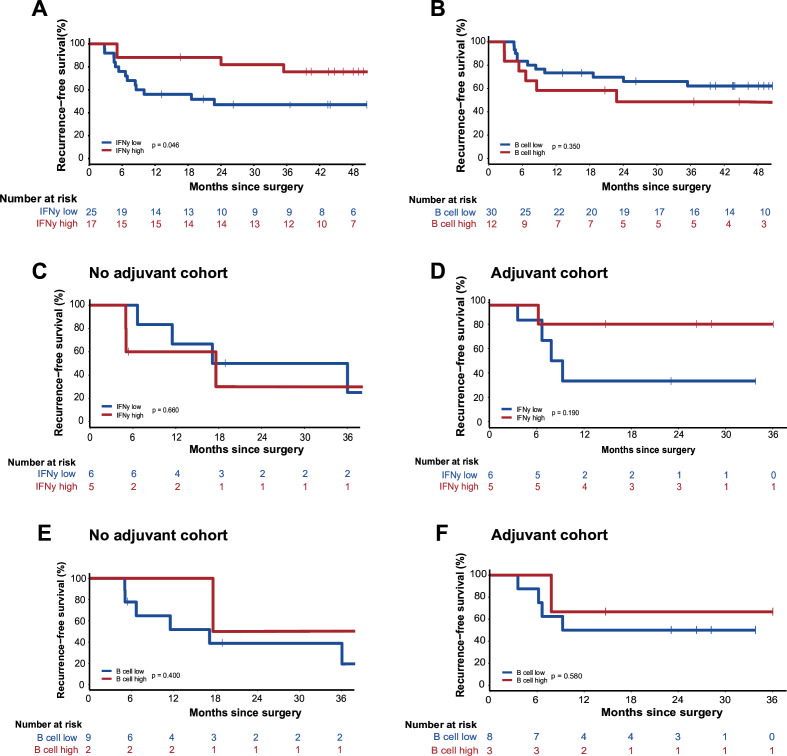
Results: After a median follow-up of 26 months of the 98 patients in our discovery set, median recurrence-free survival (RFS) was significantly longer for the adjuvant intention cohort (cohort 2, n=49) versus the observation cohort (cohort 1, n=49). Median overall survival was not reached for either cohort, nor significantly different. In observation cohort 1A (n=24), RFS was significantly longer for patients with high interferon-gamma (IFNγ) score (p=0.002); for adjuvant patients of cohort 2A (n=24), a similar trend was observed (p=0.086). Patients with high B cell score had a longer RFS in cohort 1A, but no difference was seen in cohort 2A. The B cell score based on RNA correlated with CD20+ cells in tumor area but was not independent from the IFNγ score. In the MIA validation cohort (n=44), longer RFS was observed for patients with high IFNγ score compared with low IFNγ score (p=0.046), no difference in RFS was observed according to the B cell score. In both the observation (n=11) and the adjuvant (n=11) UMCU validation cohorts, no difference in RFS was seen for IFNγ and B cell.
Conclusions: IFNγ has shown to be a prognostic marker in both patients who were and were not treated with adjuvant therapy. B cell score was prognostic but did not improve accuracy over IFNγ. Our study confirmed RFS benefit of adjuvant anti-PD-1 for patients with macroscopic stage III melanoma.
Keywords: Adjuvant Drug Therapy; Immune Checkpoint Inhibitor; Melanoma; Tumor Biomarkers.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: PD reported financial interest in Signature Oncology and will receive some possible revenues if the IFN-γ signature is being developed as a clinical companion diagnostic. AMM is a consultant advisor for BMS, MSD, Novartis, Roche, Pierre-Fabre, and QBiotics. RAS has received fees for professional services from MetaOptima Technology Inc., F. Hoffmann-La Roche Ltd, Evaxion, Provectus Biopharmaceuticals Australia, QBiotics, Novartis, Merck Sharp & Dohme, NeraCare, AMGEN Inc., Bristol-Myers Squibb, Myriad Genetics, GlaxoSmithKline. KPMS is consult advisor for Bristol-Myers Squibb, Merck Sharp and Dome, Abbvie, Pierre Fabre, Novartis, and Sairopa; has received honoraria from Novartis, Roche, Merck Sharp, and Dome; and has received research funding from TigaTx, Bristol Myers Squibb, and Philips; all paid to the institute. GVL is a consultant advisor for Agenus, Amgen, Array Biopharma, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Evaxion, Hexal AG (Sandoz Company), Highlight Therapeutics S.L., Innovent Biologics USA, Merck Sharpe & Dohme, Novartis, OncoSec, PHMR Ltd, Pierre Fabre, Provectus, QBiotics, and Regeneron. ACJvA has received advisory board and consultancy honoraria from Amgen, Bristol-Myers Squibb, Novartis, MSD-Merck, Merck-Pfizer, Pierre Fabre, Provectus, Sanofi, and 4SC, all paid to the institute; and research grants received from Amgen, Bristol-Myers Squibb, Merck-Pfizer, and Novartis, all paid to the institute. CB received compensation (all paid to the institute except TRV) for advisory roles for Bristol-Myers Squibb, MSD, Roche, Novartis, GSK, AZ, Pfizer, Lilly, GenMab, Pierre Fabre, and Third Rock Ventures; received research funding (all paid to the institute) from Bristol-Myers Squibb, Novartis, and NanoString, and declares stockownership in Immagene BV, where he is cofounder. All remaining authors have declared no conflicts of interest.
Figures
References
-
- Ascierto PA, Del Vecchio M, Mandalá M, et al. . Adjuvant nivolumab versus ipilimumab in resected stage IIIB-C and stage IV melanoma (Checkmate 238): 4-year results from a multicentre, double-blind, randomised, controlled, phase 3 trial. Lancet Oncol 2020;21:1465–77. 10.1016/S1470-2045(20)30494-0 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical