

Demographical and Epidemiological Contribution to Cancer Incidence in Delhi and Its Trends from 1991-2015
- PMID: 38679980
- PMCID: PMC11162734
- DOI: 10.31557/APJCP.2024.25.4.1213
Demographical and Epidemiological Contribution to Cancer Incidence in Delhi and Its Trends from 1991-2015
Abstract
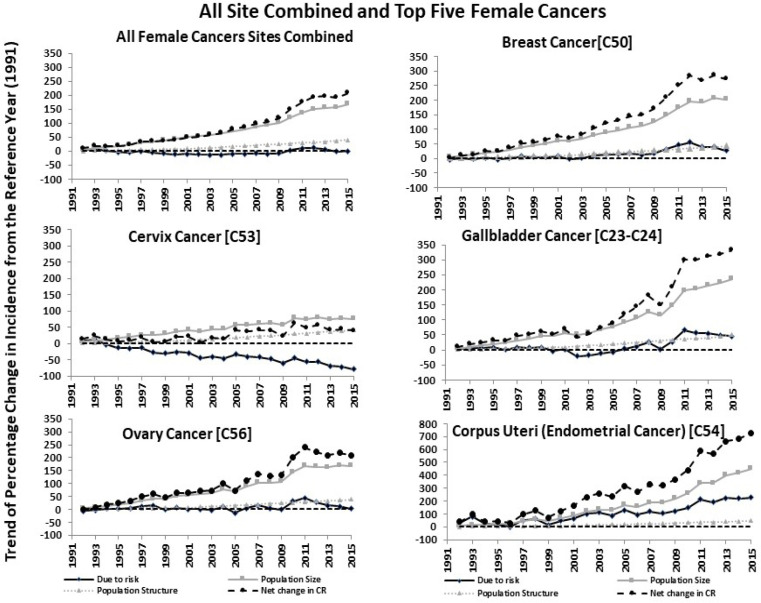
Introduction: Cancer incidences are rising worldwide, and India ranked third globally in cancer incidence as of 2020, according to estimates from GLOBOCAN. The three components that contributed to changes in cancer incidence include cancer-related risk factors, population size, and population structure. The present study aim is to derive the contribution of these factors to cancer incidence and to evaluate their trend from 1991 to 2015.
Methods: The Data were extracted from the Delhi population-based cancer registry published reports. This longstanding registry covers nearly 100% of the Delhi population. The secular trends of cancer incidence from 1991-2015 were assessed for all sites combined as well as top-five cancer sites among males and females. Joinpoint regression and Riskdiff software were performed to assess the trend among the components of cancer incidence change.
Results: Both males and females exhibited nearly equal age-standardised incidence rates over 25 years. Albeit, an overall trend in age-standardised rate was not significant for both sexes (0.68% for males and -0.16% for females) when considering all cancer sites combined. Lung, prostate, oral, and gallbladder cancer exhibits a significant rising trend in the age-standardised rates in males while in females only breast and endometrial cancer showed a rising trend. The cancer counts surged by 252% in males and 208.5% in females from 1991 to 2015. The population size component contributed a 180% increase in males and a 170% increase in females, respectively. The site-specific risk changes were more than 100% for the prostate, oral, and gallbladder cancers in males and endometrial cancer in females. The population structure (aging) contributed to rising cancer incidence varying from 35% to 60% in both genders.
Conclusion: A significant contribution to new cancer cases was observed due to a demographical shift in both population size and structure, in addition to plausible cancer-specific risk factors. This transformation could surge a potential burden on the Delhi healthcare system. Persistent endeavours are essential to expand and enhance the existing cancer care infrastructure to meet the rising demand driven by aging and population growth. Implementing a stringent population policy can help to mitigate the impact of population growth on cancer incidence.
Keywords: Delhi; Incidence; age-standardised incidence rate; cancer; epidemiological.
Conflict of interest statement
There is no conflict of interest among the authors.
Figures



Similar articles
-
Gallbladder cancer incidence in Delhi urban: A 25-year trend analysis.Indian J Cancer. 2017 Oct-Dec;54(4):673-677. doi: 10.4103/ijc.IJC_393_17. Indian J Cancer. 2017. PMID: 30082556
-
Trends in Lung Cancer Incidence in Delhi, India 1988-2012: Age-Period-Cohort and Joinpoint Analyses.Asian Pac J Cancer Prev. 2018 Jun 25;19(6):1647-1654. doi: 10.22034/APJCP.2018.19.6.1647. Asian Pac J Cancer Prev. 2018. PMID: 29937537 Free PMC article.
-
Italian cancer figures, report 2012: Cancer in children and adolescents.Epidemiol Prev. 2013 Jan-Feb;37(1 Suppl 1):1-225. Epidemiol Prev. 2013. PMID: 23585445 English, Italian.
-
[SENTIERI - Epidemiological Study of Residents in National Priority Contaminated Sites. Sixth Report].Epidemiol Prev. 2023 Jan-Apr;47(1-2 Suppl 1):1-286. doi: 10.19191/EP23.1-2-S1.003. Epidemiol Prev. 2023. PMID: 36825373 Italian.
-
Cancer trends in India: A review of population-based cancer registries (2005-2014).Indian J Public Health. 2018 Jul-Sep;62(3):221-223. doi: 10.4103/ijph.IJPH_115_17. Indian J Public Health. 2018. PMID: 30232973 Review.
Cited by
-
The impact of oxidative stress and the NRF2-KEAP1-ARE signaling pathway on anticancer drug resistance.Oncol Res. 2025 Jul 18;33(8):1819-1834. doi: 10.32604/or.2025.065755. eCollection 2025. Oncol Res. 2025. PMID: 40746900 Free PMC article. Review.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical