

Teneligliptin mitigates diabetic cardiomyopathy by inhibiting activation of the NLRP3 inflammasome
- PMID: 38680706
- PMCID: PMC11045420
- DOI: 10.4239/wjd.v15.i4.724
Teneligliptin mitigates diabetic cardiomyopathy by inhibiting activation of the NLRP3 inflammasome
Abstract
Background: Diabetic cardiomyopathy (DCM), which is a complication of diabetes, poses a great threat to public health. Recent studies have confirmed the role of NLRP3 (NOD-like receptor protein 3) activation in DCM development through the inflammatory response. Teneligliptin is an oral hypoglycemic dipeptidyl peptidase-IV inhibitor used to treat diabetes. Teneligliptin has recently been reported to have anti-inflammatory and protective effects on myocardial cells.
Aim: To examine the therapeutic effects of teneligliptin on DCM in diabetic mice.
Methods: Streptozotocin was administered to induce diabetes in mice, followed by treatment with 30 mg/kg teneligliptin.
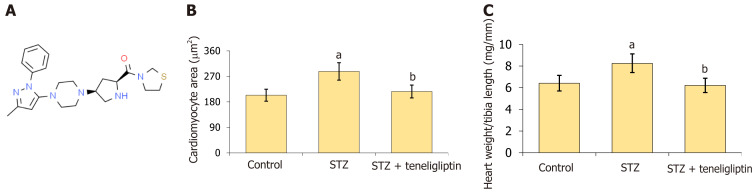
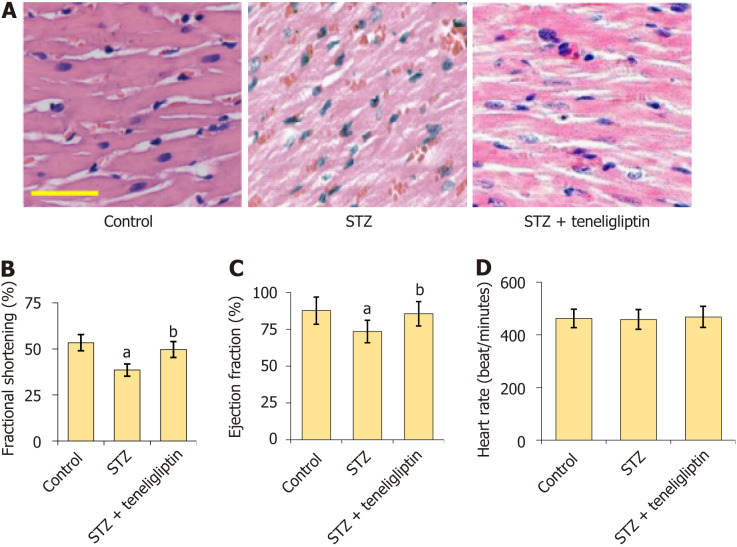
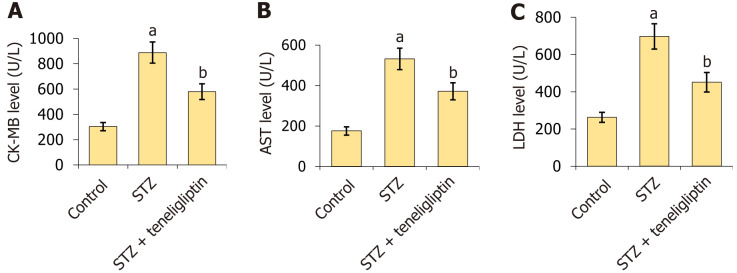
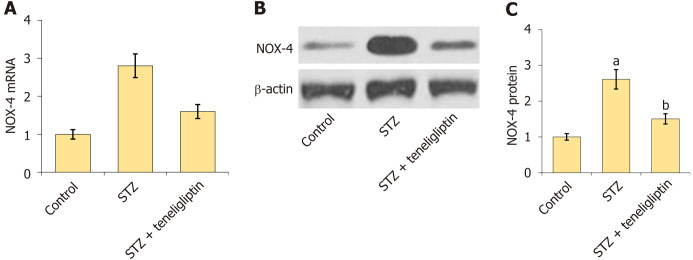
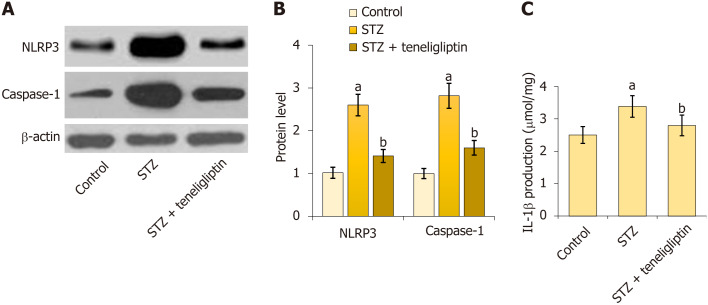
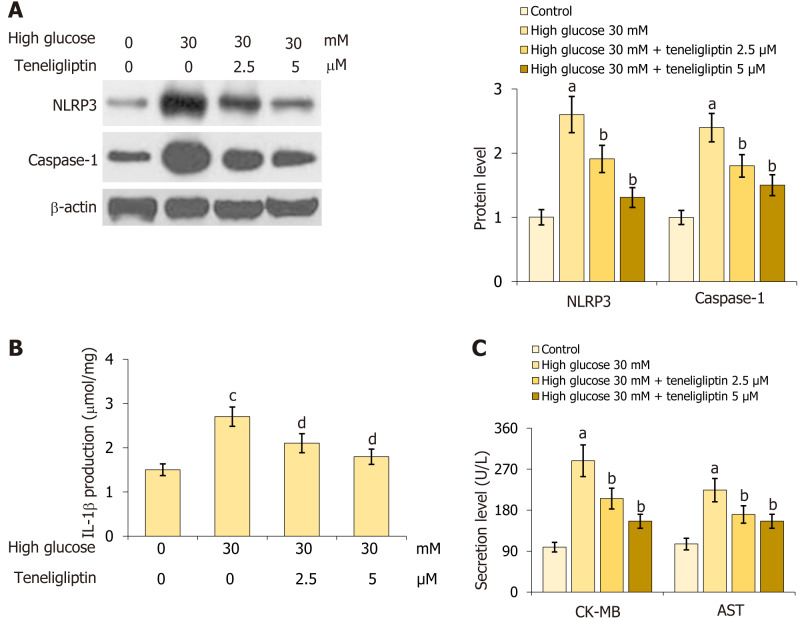
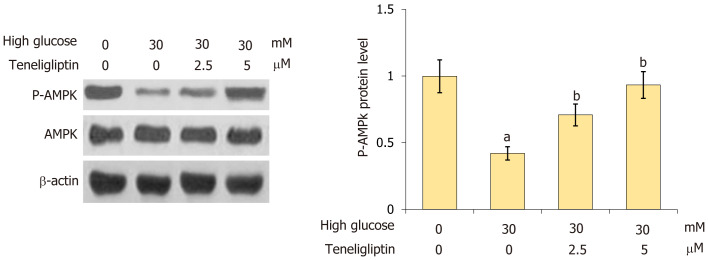
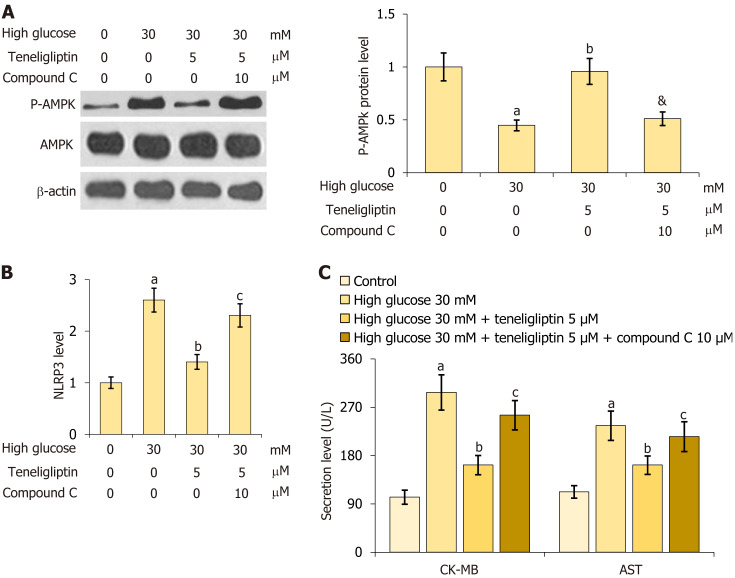
Results: Marked increases in cardiomyocyte area and cardiac hypertrophy indicator heart weight/tibia length reductions in fractional shortening, ejection fraction, and heart rate; increases in creatine kinase-MB (CK-MB), aspartate transaminase (AST), and lactate dehydrogenase (LDH) levels; and upregulated NADPH oxidase 4 were observed in diabetic mice, all of which were significantly reversed by teneligliptin. Moreover, NLRP3 inflammasome activation and increased release of interleukin-1β in diabetic mice were inhibited by teneligliptin. Primary mouse cardiomyocytes were treated with high glucose (30 mmol/L) with or without teneligliptin (2.5 or 5 µM) for 24 h. NLRP3 inflammasome activation. Increases in CK-MB, AST, and LDH levels in glucose-stimulated cardiomyocytes were markedly inhibited by teneligliptin, and AMP (p-adenosine 5'-monophosphate)-p-AMPK (activated protein kinase) levels were increased. Furthermore, the beneficial effects of teneligliptin on hyperglycaemia-induced cardiomyocytes were abolished by the AMPK signaling inhibitor compound C.
Conclusion: Overall, teneligliptin mitigated DCM by mitigating activation of the NLRP3 inflammasome.
Keywords: AMPK; Diabetic cardiomyopathy; Interleukin-1β; NLRP3; Teneligliptin.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the Authors declare that they have no conflicts of interest related to this manuscript.
Figures
References
-
- Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, Stein C, Basit A, Chan JCN, Claude Mbanya J, Pavkov ME, Ramachandaran A, Wild SH, James S, Herman WH, Zhang P, Bommer C, Kuo S, Boyko EJ, Magliano DJ. Erratum to "IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045" [Diabetes Res. Clin. Pract. 183 (2022) 109119] Diabetes Res Clin Pract. 2023;204:110945. - PubMed
-
- Japp AG, Gulati A, Cook SA, Cowie MR, Prasad SK. The Diagnosis and Evaluation of Dilated Cardiomyopathy. J Am Coll Cardiol. 2016;67:2996–3010. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
