

Contemporary trends in the incidence and timing of spinal metastases: A population-based study
- PMID: 38680988
- PMCID: PMC11046986
- DOI: 10.1093/noajnl/vdae051
Contemporary trends in the incidence and timing of spinal metastases: A population-based study
Abstract
Background: Spinal metastases are a significant complication of advanced cancer. In this study, we assess temporal trends in the incidence and timing of spinal metastases and examine underlying patient demographics and primary cancer associations.
Methods: In this population-based retrospective cohort study, health data from 2007 to 2019 in Ontario, Canada were analyzed (n = 37, 375 patients identified with spine metastases). Primary outcomes were annual incidence of spinal metastasis, and time to metastasis after primary diagnosis.
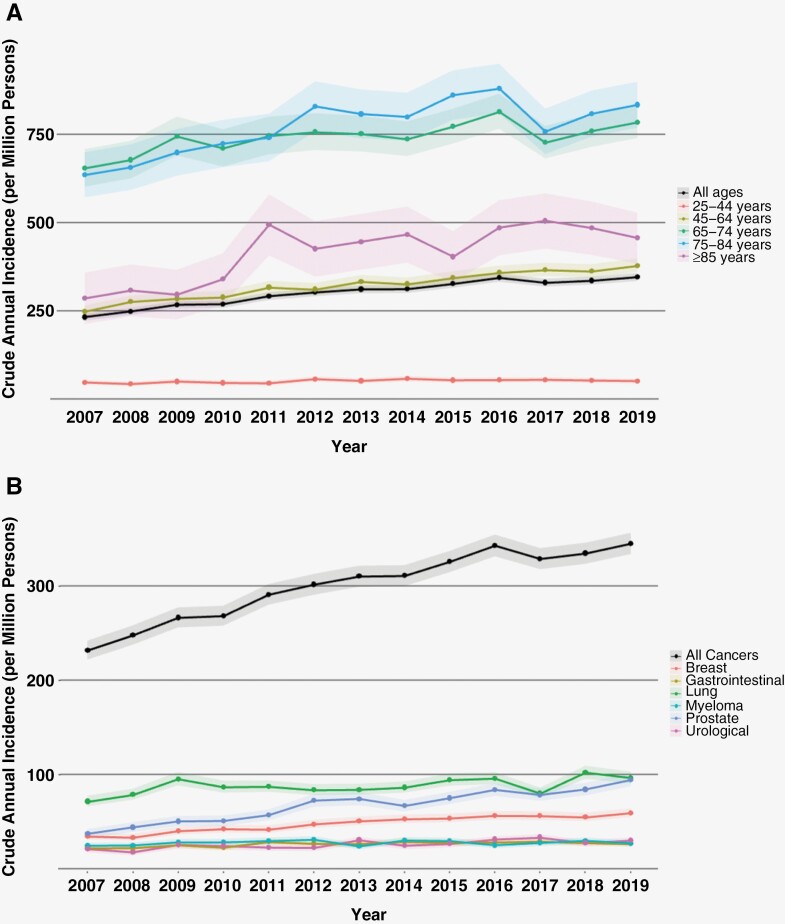
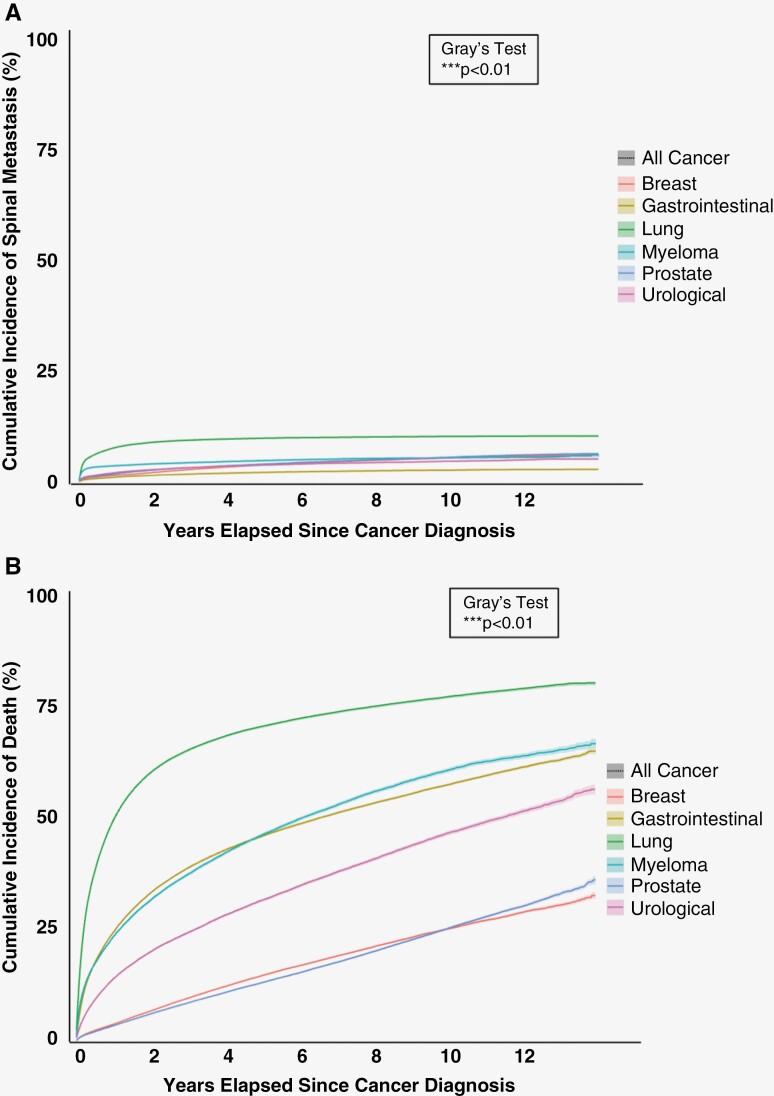
Results: The age-standardized incidence of spinal metastases increased from 229 to 302 cases per million over the 13-year study period. The average annual percent change (AAPC) in incidence was 2.2% (95% CI: 1.4% to 3.0%) with patients aged ≥85 years demonstrating the largest increase (AAPC 5.2%; 95% CI: 2.3% to 8.3%). Lung cancer had the greatest annual incidence, while prostate cancer had the greatest increase in annual incidence (AAPC 6.5; 95% CI: 4.1% to 9.0%). Lung cancer patients were found to have the highest risk of spine metastasis with 10.3% (95% CI: 10.1% to 10.5%) of patients being diagnosed at 10 years. Gastrointestinal cancer patients were found to have the lowest risk of spine metastasis with 1.0% (95% CI: 0.9% to 1.0%) of patients being diagnosed at 10 years.
Conclusions: The incidence of spinal metastases has increased in recent years, particularly among older patients. The incidence and timing vary substantially among different primary cancer types. These findings contribute to the understanding of disease trends and emphasize a growing population of patients who require subspecialty care.
Keywords: Ontario; cohort studies; epidemiology; incidence; spinal metastasis.
© The Author(s) 2024. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
No authors reported conflicts of interest related to this study. Outside of this study, AS has been a consultant for Varian, Elekta (Gamma Knife Icon), BrainLAB, Merck, Abbvie, and Roche; Vice President of the International Stereotactic Radiosurgery Society (ISRS); Co-Chair of the AO Spine Knowledge Forum Tumor; received honorarium for past educational seminars for AstraZeneca, Elekta AB, Varian, BrainLAB, Accuray, Seagen Inc.; research grant with Elekta AB, Varian, Seagen Inc., BrainLAB; and travel accommodations/expenses with Elekta, Varian, and BrainLAB. AS also belongs to the Elekta MR Linac Research Consortium and is a Clinical Steering Committee Member, and chairs the Elekta Oligometastases Group and the Elekta Gamma Knife Icon Group outside of this study. ND reported personal feeds from Stryker, Medtronic, Cerapedics, and Baxter outside the submitted work. ND is a stockholder of Medtronic and received fellowship support from Medtronic, AOSpine, and JJ/Synthes outside the submitted work. CDW reported grants from Cerapedics and personal fees from Stryker outside the submitted work. DAR reported research support from a Canada Research Chair in Medical Decision Sciences, the Canadian Institutes of Health Research, the PSI Foundation of Ontario, and the Kimel-Schatzky Traumatic Brain Injury Research Fund outside the submitted work. JRW reported personal fees from Stryker Canada outside the submitted work.
Figures
References
-
- Nater A, Sahgal A, Fehlings M.. Chapter 16 - Management - spinal metastases. Handb Clin Neurol. 2018;149:239–255. - PubMed
-
- Fehlings MG, Nater A, Holmer H.. Cost-effectiveness of surgery in the management of metastatic epidural spinal cord compression: A systematic review. Spine (Phila Pa 1976). 2014;39(22):S99–S105. - PubMed
-
- Nater A, Chuang J, Liu K, et al. A personalized medicine approach for the management of spinal metastases with cord compression: Development of a novel clinical prediction model for postoperative survival and quality of life. World Neurosurg. 2020;140:654–663.e13. - PubMed
-
- Nater A, Tetreault LA, Kopjar B, et al. Predictive factors of survival in a surgical series of metastatic epidural spinal cord compression and complete external validation of 8 multivariate models of survival in a prospective North American multicenter study. Cancer. 2018;124(17):3536–3550. - PubMed
-
- Siegel RL, Miller KD, Wagle NS, Jemal A.. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. - PubMed
LinkOut - more resources
Full Text Sources