

Early, precise, and safe clinical evaluation of the pharmacodynamic effects of novel agents in the intact human tumor microenvironment
- PMID: 38681192
- PMCID: PMC11048044
- DOI: 10.3389/fphar.2024.1367581
Early, precise, and safe clinical evaluation of the pharmacodynamic effects of novel agents in the intact human tumor microenvironment
Abstract
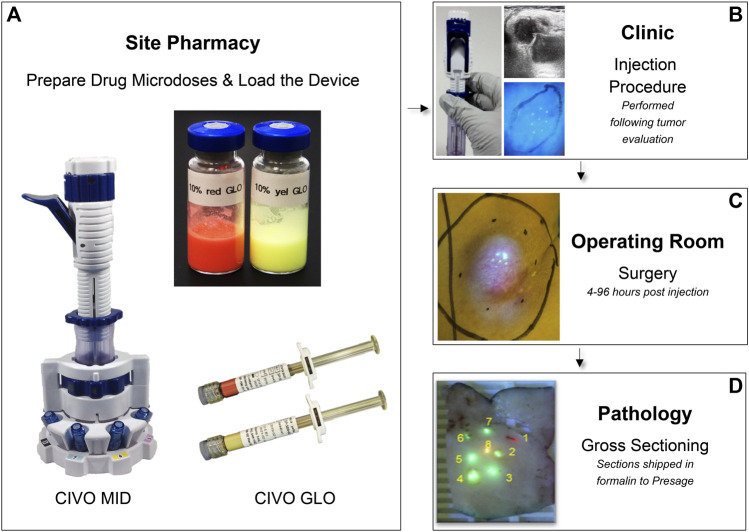
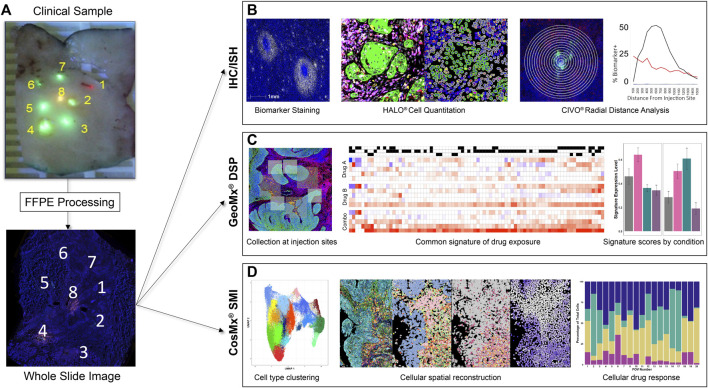
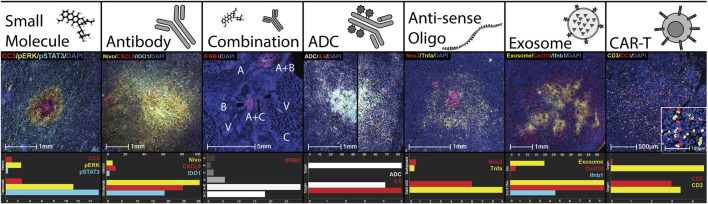
Introduction: Drug development is systemically inefficient. Research and development costs for novel therapeutics average hundreds of millions to billions of dollars, with the overall likelihood of approval estimated to be as low as 6.7% for oncology drugs. Over half of these failures are due to a lack of drug efficacy. This pervasive and repeated low rate of success exemplifies how preclinical models fail to adequately replicate the complexity and heterogeneity of human cancer. Therefore, new methods of evaluation, early in the development trajectory, are essential both to rule-in and rule-out novel agents with more rigor and speed, but also to spare clinical trial patients from the potentially toxic sequelae (high risk) of testing investigational agents that have a low likelihood of producing a response (low benefit). Methods: The clinical in vivo oncology (CIVO®) platform was designed to change this drug development paradigm. CIVO precisely delivers microdose quantities of up to 8 drugs or combinations directly into patient tumors 4-96 h prior to planned surgical resection. Resected tissue is then analyzed for responses at each site of intratumoral drug exposure. Results: To date, CIVO has been used safely in 6 clinical trials, including 68 subjects, with 5 investigational and 17 approved agents. Resected tissues were analyzed initially using immunohistochemistry and in situ hybridization assays (115 biomarkers). As technology advanced, the platform was paired with spatial biology analysis platforms, to successfully track anti-neoplastic and immune-modulating activity of the injected agents in the intact tumor microenvironment. Discussion: Herein we provide a report of the use of CIVO technology in patients, a depiction of the robust analysis methods enabled by this platform, and a description of the operational and regulatory mechanisms used to deploy this approach in synergistic partnership with pharmaceutical partners. We further detail how use of the CIVO platform is a clinically safe and scientifically precise alternative or complement to preclinical efficacy modeling, with outputs that inform, streamline, and de-risk drug development.
Keywords: drug development; intratumoral microdosing; multidrug analyses; pharmacodynamics; phase 0; spatial profiling; tumor microenvironment.
Copyright © 2024 Gundle, Rajasekaran, Houlton, Deutsch, Ow, Maki, Pang, Nathan, Clayburgh, Newman, Brinkmann, Wagner, Pollack, Thompson, Li, Mehta, Schiff, Wenig, Swiecicki, Tang, Davis, van Zante, Bertout, Jenkins, Turner, Grenley, Burns, Frazier, Merrell, Sottero, Derry, Gillespie, Mills and Klinghoffer.
Conflict of interest statement
WJ, AT, and BM are employees of Presage Biosciences, Inc. CB, AM, KS, KCG, JB, MG, JF, JD, and RK are employees of and hold ownership interest (including patents (MG, JF, and RK)) in Presage Biosciences. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare that this study (NCT04065555 and NCT06062602) received funding from Takeda Pharmaceuticals. The funder had the following involvement: study design, supply of drug, and the review of this article. The authors declare that this study (NCT04272333) received funding from Celgene Corporation. The funder had the following involvement: study design and supply of study drug. The authors declare that this study (NCT04541108) received funding from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. The funder had the following involvement: study design, supply of study drug, and the review of this article.
Figures
Similar articles
-
Trackable Intratumor Microdosing and Spatial Profiling Provide Early Insights into Activity of Investigational Agents in the Intact Tumor Microenvironment.Clin Cancer Res. 2023 Sep 15;29(18):3813-3825. doi: 10.1158/1078-0432.CCR-23-0827. Clin Cancer Res. 2023. PMID: 37389981 Free PMC article. Clinical Trial.
-
A technology platform to assess multiple cancer agents simultaneously within a patient's tumor.Sci Transl Med. 2015 Apr 22;7(284):284ra58. doi: 10.1126/scitranslmed.aaa7489. Sci Transl Med. 2015. PMID: 25904742 Free PMC article.
-
Multiplexed Evaluation of Microdosed Antineoplastic Agents In Situ in the Tumor Microenvironment of Patients with Soft Tissue Sarcoma.Clin Cancer Res. 2020 Aug 1;26(15):3958-3968. doi: 10.1158/1078-0432.CCR-20-0614. Epub 2020 Apr 16. Clin Cancer Res. 2020. PMID: 32299817
-
Efaproxiral: GSJ 61, JP 4, KDD 86, RS 4, RSR 13.Drugs R D. 2005;6(3):178-85. doi: 10.2165/00126839-200506030-00007. Drugs R D. 2005. PMID: 15869322 Review.
-
Biomarker-driven early clinical trials in oncology: a paradigm shift in drug development.Cancer J. 2009 Sep-Oct;15(5):406-20. doi: 10.1097/PPO.0b013e3181bd0445. Cancer J. 2009. PMID: 19826361 Review.
Cited by
-
Ubiquitination and deubiquitination in cancer: from mechanisms to novel therapeutic approaches.Mol Cancer. 2024 Jul 25;23(1):148. doi: 10.1186/s12943-024-02046-3. Mol Cancer. 2024. PMID: 39048965 Free PMC article. Review.
References
-
- Derry J. M. J., Burns C., Frazier J. P., Beirne E., Grenley M., DuFort C. C., et al. (2023). Trackable intratumor microdosing and spatial profiling provide early insights into activity of investigational agents in the intact tumor microenvironment. Clin. Cancer Res. 29, 3813–3825. 10.1158/1078-0432.CCR-23-0827 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials