

Effects of positive end-expiratory pressure on intracranial pressure, cerebral perfusion pressure, and brain oxygenation in acute brain injury: Friend or foe? A scoping review
- PMID: 38681785
- PMCID: PMC11043646
- DOI: 10.1016/j.jointm.2023.08.001
Effects of positive end-expiratory pressure on intracranial pressure, cerebral perfusion pressure, and brain oxygenation in acute brain injury: Friend or foe? A scoping review
Abstract
Background: Patients with acute brain injury (ABI) are a peculiar population because ABI does not only affect the brain but also other organs such as the lungs, as theorized in brain-lung crosstalk models. ABI patients often require mechanical ventilation (MV) to avoid the complications of impaired respiratory function that can follow ABI; MV should be settled with meticulousness owing to its effects on the intracranial compartment, especially regarding positive end-expiratory pressure (PEEP). This scoping review aimed to (1) describe the physiological basis and mechanisms related to the effects of PEEP in ABI; (2) examine how clinical research is conducted on this topic; (3) identify methods for setting PEEP in ABI; and (4) investigate the impact of the application of PEEP in ABI on the outcome.
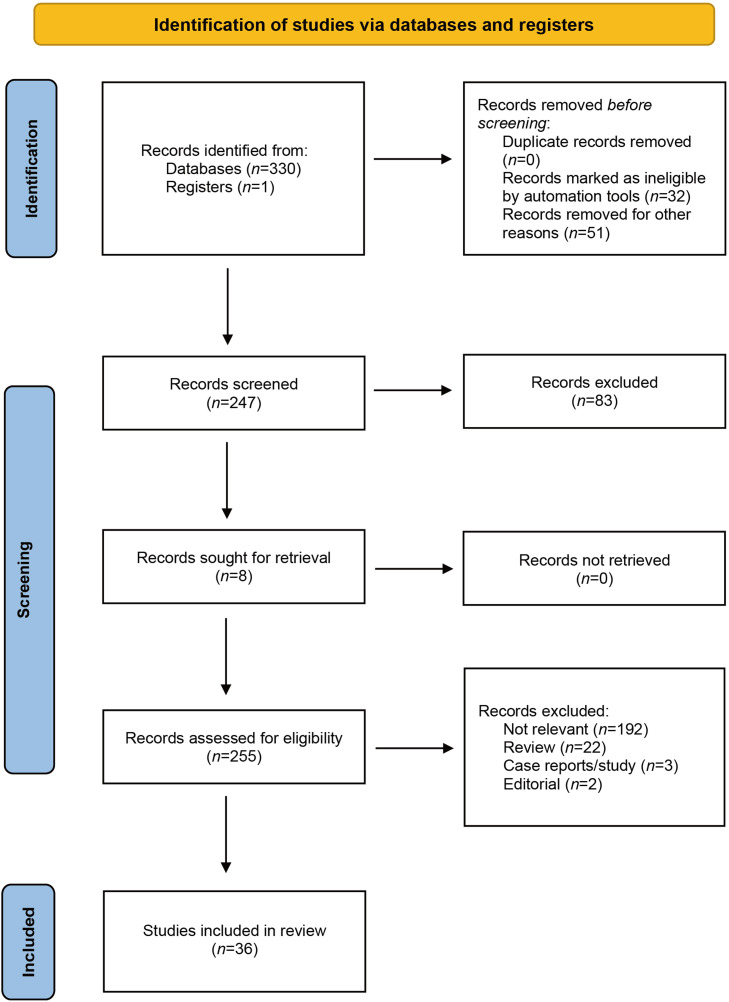
Methods: The five-stage paradigm devised by Peters et al. and expanded by Arksey and O'Malley, Levac et al., and the Joanna Briggs Institute was used for methodology. We also adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension criteria. Inclusion criteria: we compiled all scientific data from peer-reviewed journals and studies that discussed the application of PEEP and its impact on intracranial pressure, cerebral perfusion pressure, and brain oxygenation in adult patients with ABI. Exclusion criteria: studies that only examined a pediatric patient group (those under the age of 18), experiments conducted solely on animals; studies without intracranial pressure and/or cerebral perfusion pressure determinations, and studies with incomplete information. Two authors searched and screened for inclusion in papers published up to July 2023 using the PubMed-indexed online database. Data were presented in narrative and tubular form.
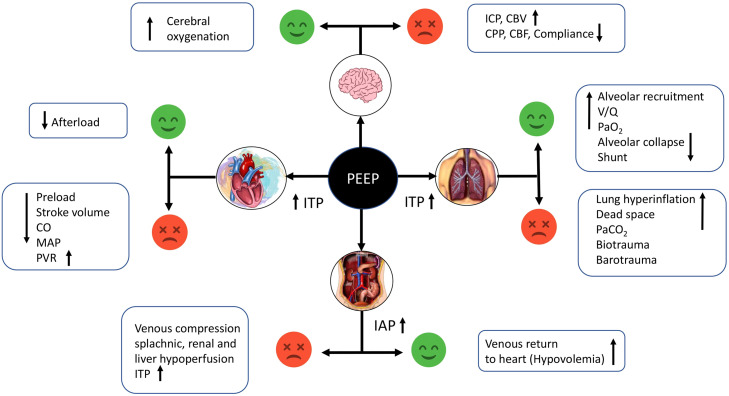
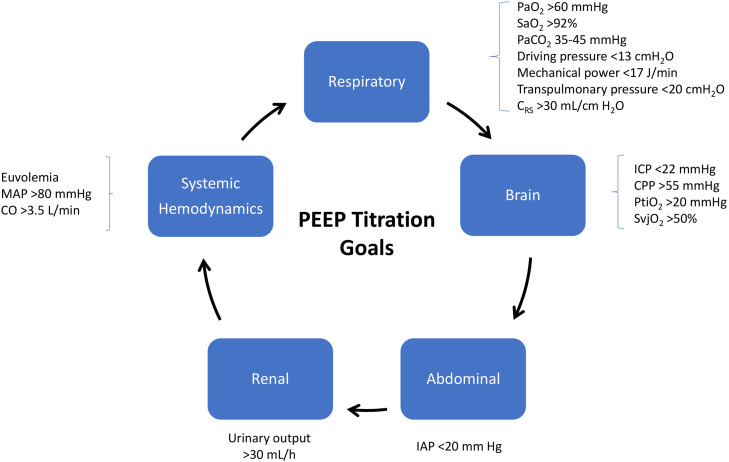
Results: The initial search yielded 330 references on the application of PEEP in ABI, of which 36 met our inclusion criteria. PEEP has recognized beneficial effects on gas exchange, but it produces hemodynamic changes that should be predicted to avoid undesired consequences on cerebral blood flow and intracranial pressure. Moreover, the elastic properties of the lungs influence the transmission of the forces applied by MV over the brain so they should be taken into consideration. Currently, there are no specific tools that can predict the effect of PEEP on the brain, but there is an established need for a comprehensive monitoring approach for these patients, acknowledging the etiology of ABI and the measurable variables to personalize MV.
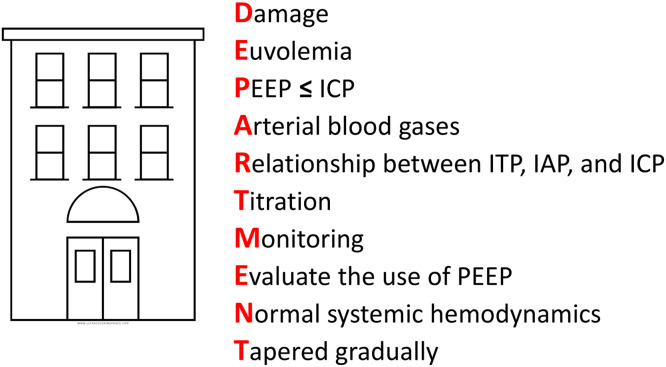
Conclusion: PEEP can be safely used in patients with ABI to improve gas exchange keeping in mind its potentially harmful effects, which can be predicted with adequate monitoring supported by bedside non-invasive neuromonitoring tools.
Keywords: Acute brain injury; Brain–lung crosstalk; Intracranial pressure; Mechanical ventilation; Multimodal monitoring; Positive end-expiratory pressure.
© 2023 The Author(s).
Figures
Similar articles
-
Intracranial response to positive end-expiratory pressure is influenced by lung recruitability and gas distribution during mechanical ventilation in acute brain injury patients: a proof-of-concept physiological study.Intensive Care Med Exp. 2025 Apr 14;13(1):43. doi: 10.1186/s40635-025-00750-y. Intensive Care Med Exp. 2025. PMID: 40229445 Free PMC article.
-
Effects of positive end-expiratory pressure on brain oxygenation, systemic oxygen cascade and metabolism in acute brain injured patients: a pilot physiological cross-sectional study.J Clin Monit Comput. 2024 Feb;38(1):165-175. doi: 10.1007/s10877-023-01042-0. Epub 2023 Jul 15. J Clin Monit Comput. 2024. PMID: 37453007
-
Effects of positive end-expiratory pressure on regional cerebral blood flow, intracranial pressure, and brain tissue oxygenation.Crit Care Med. 2005 Oct;33(10):2367-72. doi: 10.1097/01.ccm.0000181732.37319.df. Crit Care Med. 2005. PMID: 16215394 Clinical Trial.
-
Positive end-expiratory pressure for preterm infants requiring conventional mechanical ventilation for respiratory distress syndrome or bronchopulmonary dysplasia.Cochrane Database Syst Rev. 2019 Feb 26;2(2):CD004500. doi: 10.1002/14651858.CD004500.pub3. Cochrane Database Syst Rev. 2019. PMID: 30820939 Free PMC article.
-
Methods for determining optimal positive end-expiratory pressure in patients undergoing invasive mechanical ventilation: a scoping review.Can J Anaesth. 2024 Nov;71(11):1535-1555. doi: 10.1007/s12630-024-02871-6. Epub 2024 Nov 20. Can J Anaesth. 2024. PMID: 39565498 Free PMC article.
Cited by
-
Critical upward shift of intracranial pressure levels in extremely obese patients; normalization due to bariatric surgery.Ultrasound J. 2025 Jul 28;17(1):35. doi: 10.1186/s13089-025-00439-z. Ultrasound J. 2025. PMID: 40719929 Free PMC article.
-
Does helmet CPAP reduce carotid flow compared to oronasal mask CPAP? A randomized cross-over trial in healthy subjects.Intern Emerg Med. 2025 Mar 12. doi: 10.1007/s11739-025-03914-6. Online ahead of print. Intern Emerg Med. 2025. PMID: 40072680
-
Lung Ultrasound in Mechanical Ventilation: A Purposive Review.Diagnostics (Basel). 2025 Mar 28;15(7):870. doi: 10.3390/diagnostics15070870. Diagnostics (Basel). 2025. PMID: 40218220 Free PMC article. Review.
-
Impact of healthcare system strain on the implementation of ICU sedation practices and encephalopathy burden during the early COVID-19 pandemic.Geroscience. 2025 Feb;47(1):189-203. doi: 10.1007/s11357-024-01336-4. Epub 2024 Sep 7. Geroscience. 2025. PMID: 39243283 Free PMC article.
-
Intracranial response to positive end-expiratory pressure is influenced by lung recruitability and gas distribution during mechanical ventilation in acute brain injury patients: a proof-of-concept physiological study.Intensive Care Med Exp. 2025 Apr 14;13(1):43. doi: 10.1186/s40635-025-00750-y. Intensive Care Med Exp. 2025. PMID: 40229445 Free PMC article.
References
-
- Del Sorbo L., Goligher E.C., McAuley D.F., Rubenfeld G.D., Brochard L.J., Gattinoni L., et al. Mechanical ventilation in adults with acute respiratory distress syndrome. Summary of the experimental evidence for the clinical practice guideline. Ann Am Thorac Soc. 2017;14 doi: 10.1513/AnnalsATS.201704-345OT. Supplement_4S261-261S270. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
