

Latest developments in early diagnosis and specific treatment of severe influenza infection
- PMID: 38681787
- PMCID: PMC11043645
- DOI: 10.1016/j.jointm.2023.09.006
Latest developments in early diagnosis and specific treatment of severe influenza infection
Abstract
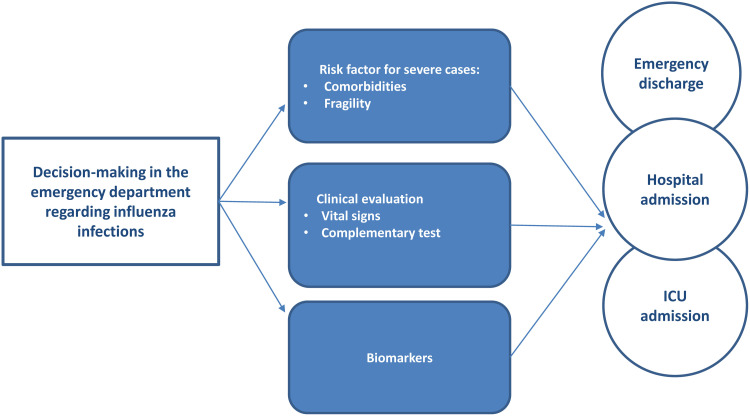
Influenza pandemics are unpredictable recurrent events with global health, economic, and social consequences. The objective of this review is to provide an update on the latest developments in early diagnosis and specific treatment of the disease and its complications, particularly with regard to respiratory organ failure. Despite advances in treatment, the rate of mortality in the intensive care unit remains approximately 30%. Therefore, early identification of potentially severe viral pneumonia is extremely important to optimize treatment in these patients. The pathogenesis of influenza virus infection depends on viral virulence and host response. Thus, in some patients, it is associated with an excessive systemic response mediated by an authentic cytokine storm. This process leads to severe primary pneumonia and acute respiratory distress syndrome. Initial prognostication in the emergency department based on comorbidities, vital signs, and biomarkers (e.g., procalcitonin, ferritin, human leukocyte antigen-DR, mid-regional proadrenomedullin, and lactate) is important. Identification of these biomarkers on admission may facilitate clinical decision-making to determine early admission to the hospital or the intensive care unit. These decisions are reached considering pathophysiological circumstances that are associated with a poor prognosis (e.g., bacterial co-infection, hyperinflammation, immune paralysis, severe endothelial damage, organ dysfunction, and septic shock). Moreover, early implementation is important to increase treatment efficacy. Based on a limited level of evidence, all current guidelines recommend using oseltamivir in this setting. The possibility of drug resistance should also be considered. Alternative options include other antiviral drugs and combination therapies with monoclonal antibodies. Importantly, it is not recommended to use corticosteroids in the initial treatment of these patients. Furthermore, the implementation of supportive measures for respiratory failure is essential. Current recommendations are limited, heterogeneous, and not regularly updated. Early intubation and mechanical ventilation is the basic treatment for patients with severe respiratory failure. Prone ventilation should be promptly performed in patients with acute respiratory distress syndrome, while early tracheostomy should be considered in case of planned prolonged mechanical ventilation. Clinical trials on antiviral treatment and respiratory support measures specifically for these patients, as well as specific recommendations for different at-risk populations, are necessary to improve outcomes.
Keywords: Acute respiratory distress syndrome; Influenza; Intensive care unit admission; Pandemic; Respiratory failure.
© 2024 The Authors. Published by Elsevier B.V. on behalf of Chinese Medical Association.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




Similar articles
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
[Recommendations of the Infectious Diseases Work Group (GTEI) of the Spanish Society of Intensive and Critical Care Medicine and Coronary Units (SEMICYUC) and the Infections in Critically Ill Patients Study Group (GEIPC) of the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) for the diagnosis and treatment of influenza A/H1N1 in seriously ill adults admitted to the Intensive Care Unit].Med Intensiva. 2012 Mar;36(2):103-37. doi: 10.1016/j.medin.2011.11.020. Epub 2012 Jan 13. Med Intensiva. 2012. PMID: 22245450 Spanish.
-
Intensive care for seriously ill patients affected by novel coronavirus sars - CoV - 2: Experience of the Crema Hospital, Italy.Am J Emerg Med. 2021 Jul;45:156-161. doi: 10.1016/j.ajem.2020.08.005. Epub 2020 Aug 16. Am J Emerg Med. 2021. PMID: 33046317 Free PMC article.
-
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012.Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af. Crit Care Med. 2013. PMID: 23353941
-
Critical care management of adults with community-acquired severe respiratory viral infection.Intensive Care Med. 2020 Feb;46(2):315-328. doi: 10.1007/s00134-020-05943-5. Epub 2020 Feb 10. Intensive Care Med. 2020. PMID: 32040667 Free PMC article. Review.
Cited by
-
Impact of menopausal hormone therapy on influenza complications in women: a systematic assessment study.Ann Med. 2025 Dec;57(1):2534095. doi: 10.1080/07853890.2025.2534095. Epub 2025 Jul 17. Ann Med. 2025. PMID: 40676907 Free PMC article.
-
AI-driven early detection of severe influenza in Jiangsu, China: a deep learning model validated through the design of multi-center clinical trials and prospective real-world deployment.Front Public Health. 2025 Aug 18;13:1610244. doi: 10.3389/fpubh.2025.1610244. eCollection 2025. Front Public Health. 2025. PMID: 40900711 Free PMC article. Clinical Trial.
-
Development of an early prediction model for risk of influenza A and influenza B based on complete blood count examination.BMC Infect Dis. 2025 Sep 1;25(1):1088. doi: 10.1186/s12879-025-11502-4. BMC Infect Dis. 2025. PMID: 40890653 Free PMC article.
References
-
- Influenza (Seasonal). [Internet]. Who.int. 2019 [Access: November 9, 2023]. Available from: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal).
Publication types
LinkOut - more resources
Full Text Sources
