

Potential effects of a mobile stroke unit on time to treatment and outcome in patients treated with thrombectomy or thrombolysis: A Danish-German cross-border analysis
- PMID: 38682808
- PMCID: PMC11295161
- DOI: 10.1111/ene.16298
Potential effects of a mobile stroke unit on time to treatment and outcome in patients treated with thrombectomy or thrombolysis: A Danish-German cross-border analysis
Abstract
Background and purpose: A mobile stroke unit (MSU) reduces delays in stroke treatment by allowing thrombolysis on board and avoiding secondary transports. Due to the beneficial effect in comparison to conventional emergency medical services, current guidelines recommend regional evaluation of MSU implementation.
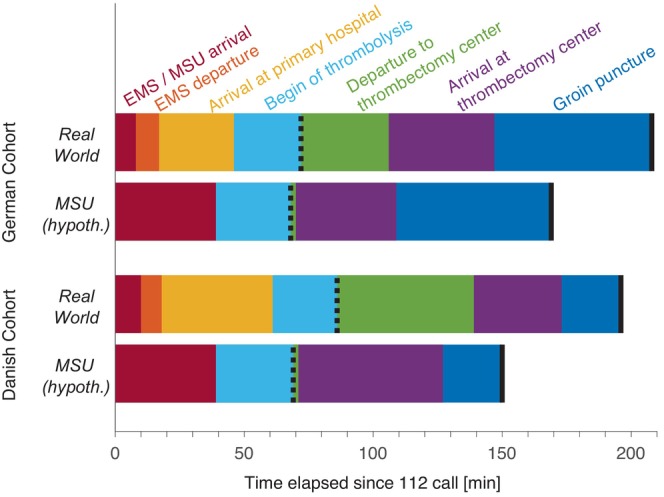
Methods: In a descriptive study, current pathways of patients requiring a secondary transport for mechanical thrombectomy were reconstructed from individual patient records within a Danish (n = 122) and an adjacent German region (n = 80). Relevant timestamps included arrival times (on site, primary hospital, thrombectomy centre) as well as the initiation of acute therapy. An optimal MSU location for each region was determined. The resulting time saving was translated into averted disability-adjusted life years (DALYs).
Results: For each region, the optimal MSU location required a median driving time of 35 min to a stroke patient. Time savings in the German region (median [Q1; Q3]) were 7 min (-15; 31) for thrombolysis and 35 min (15; 61) for thrombectomy. In the Danish region, the corresponding time savings were 20 min (8; 30) and 43 min (25; 66). Assuming 28 thrombectomy cases and 52 thrombolysis cases this would translate to 9.4 averted DALYs per year justifying an annual net MSU budget of $0.8M purchasing power parity dollars (PPP-$) in the German region. In the Danish region, the MSU would avert 17.7 DALYs, justifying an annual net budget of PPP-$1.7M.
Conclusion: The effects of an MSU can be calculated from individual patient pathways and reflect differences in the hospital infrastructure between Denmark and Germany.
Keywords: drip and ship model; mobile stroke unit; stroke; thrombectomy; thrombolysis.
© 2024 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
GR received speaker's honoraria and/or reimbursement for congress travelling and accommodation from Boehringer‐Ingelheim, Bristol‐Myers Squibb, Astra Zeneca, Ipsen, Boston Scientific, Novartis and Daiichi Sankyo.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
