

[Recent developments in acute kidney injury : Definition, biomarkers, subphenotypes, and management]
- PMID: 38683229
- PMCID: PMC11130018
- DOI: 10.1007/s00063-024-01142-y
[Recent developments in acute kidney injury : Definition, biomarkers, subphenotypes, and management]
Abstract
Acute kidney injury (AKI) is a common problem in critically ill patients and is associated with increased morbidity and mortality. Since 2012, AKI has been defined according to the KDIGO (Kidney Disease Improving Global Outcome) guidelines. As some biomarkers are now available that can provide useful clinical information, a new definition including a new stage 1S has been proposed by an expert group of the Acute Disease Quality Initiative (ADQI). At this stage, classic AKI criteria are not yet met, but biomarkers are already positive defining subclinical AKI. This stage 1S is associated with a worse patient outcome, regardless of the biomarker chosen. The PrevAKI and PrevAKI-Multicenter trial also showed that risk stratification with a biomarker and implementation of the KDIGO bundle (in the high-risk group) can reduce the rate of moderate and severe AKI. In the absence of a successful clinical trial, conservative management remains the primary focus of treatment. This mainly involves optimization of hemodynamics and an individualized (restrictive) fluid management. The STARRT-AKI trial has shown that there is no benefit from accelerated initiation of renal replacement therapy. However, delaying too long might be associated with potential harm, as shown in the AKIKI2 study. Prospective studies are needed to determine whether artificial intelligence will play a role in AKI in the future, helping to guide treatment decisions and improve outcomes.
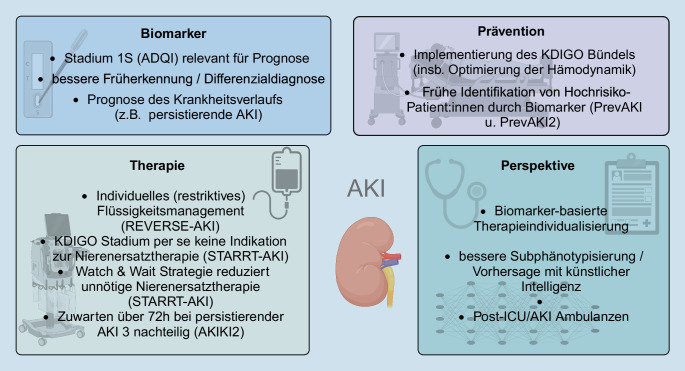
Die akute Nierenschädigung (AKI) ist v. a. bei kritisch kranken Patient:innen ein häufiges Problem, das mit einer deutlich erhöhten Morbidität und Mortalität einhergeht. Definiert ist die AKI seit 2012 nach den Leitlinien der Initiative Kidney Disease: Improving Global Outcomes (KDIGO). Da mittlerweile einige Biomarker verfügbar sind, die nützliche klinische Informationen liefern können, wurde von einer Expert:innen-Gruppe der Acute Disease Quality Initiative (ADQI) eine neue Definition unter Einbeziehung eines neuen Stadiums 1S vorgeschlagen. In diesem Stadium sind die klassischen AKI-Kriterien noch nicht erfüllt, jedoch Biomarker im Sinne eines subklinischen AKI bereits positiv, was wiederum – unabhängig vom gewählten Biomarker – bereits mit einem schlechteren Outcome assoziiert ist. In der PrevAKI- und PrevAKI-Multicenter-Studie konnte zudem gezeigt werden, dass durch eine Risikoeinstufung mithilfe eines Biomarkers und eine daran geschaltete konsequente Umsetzung des sog. KDIGO-Bündels (in der Hochrisikogruppe) die Rate an moderater und schwerer AKI reduziert werden kann. Im Bereich der Therapie steht mangels erfolgreicher klinischer Studien weiterhin das konservative Management im Vordergrund. Hier ist v. a. eine Optimierung der Hämodynamik sowie ein individuelles (eher restriktives) Flüssigkeitsmanagement zu nennen. Im Bereich der Nierenersatztherapie hat die STARRT-AKI-Studie gezeigt, dass ein beschleunigter Beginn keine Vorteile bringt. Ein zu langes Hinauszögern könnte für die Patient:innen jedoch mit einem potenziellen Schaden verbunden sein, wie in der AKIKI2-Studie gezeigt wurde. Inwiefern auch bei der AKI künstliche Intelligenz in Zukunft eine Rolle spielt, bei Therapieentscheidungen unterstützen und somit auch das Outcome von AKI-Patient:innen verbessern kann, muss noch in prospektiven Studien gezeigt werden.
Keywords: Biomarker; Kidney replacement therapie; Prevention; Renal replacement therapy; Subphenotypes.
© 2024. The Author(s).
Similar articles
-
Biomarker-guided implementation of the KDIGO guidelines to reduce the occurrence of acute kidney injury in patients after cardiac surgery (PrevAKI-multicentre): protocol for a multicentre, observational study followed by randomised controlled feasibility trial.BMJ Open. 2020 Apr 6;10(4):e034201. doi: 10.1136/bmjopen-2019-034201. BMJ Open. 2020. PMID: 32265240 Free PMC article.
-
Hierarchical endpoints in critical care: A post-hoc exploratory analysis of the standard versus accelerated initiation of renal-replacement therapy in acute kidney injury and the intensity of continuous renal-replacement therapy in critically ill patients trials.J Crit Care. 2024 Aug;82:154767. doi: 10.1016/j.jcrc.2024.154767. Epub 2024 Mar 11. J Crit Care. 2024. PMID: 38461657 Clinical Trial.
-
Peritoneal dialysis in children with sepsis-associated AKI (SA-AKI): an experience in a low- to middle-income country.Paediatr Int Child Health. 2021 May;41(2):137-144. doi: 10.1080/20469047.2021.1874201. Epub 2021 Jan 17. Paediatr Int Child Health. 2021. PMID: 33455545
-
Acute Kidney Injury: Biomarker-Guided Diagnosis and Management.Medicina (Kaunas). 2022 Feb 23;58(3):340. doi: 10.3390/medicina58030340. Medicina (Kaunas). 2022. PMID: 35334515 Free PMC article. Review.
-
Implementing the Kidney Disease: Improving Global Outcomes/acute kidney injury guidelines in ICU patients.Curr Opin Crit Care. 2013 Dec;19(6):544-53. doi: 10.1097/MCC.0000000000000039. Curr Opin Crit Care. 2013. PMID: 24240820 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
