

Safety Profile of Upadacitinib up to 5 Years in Psoriatic Arthritis, Ankylosing Spondylitis, and Non-radiographic Axial Spondyloarthritis: An Integrated Analysis of Clinical Trials
- PMID: 38683479
- PMCID: PMC11111431
- DOI: 10.1007/s40744-024-00671-4
Safety Profile of Upadacitinib up to 5 Years in Psoriatic Arthritis, Ankylosing Spondylitis, and Non-radiographic Axial Spondyloarthritis: An Integrated Analysis of Clinical Trials
Abstract
Introduction: This integrated analysis of the phase 2/3 and phase 3 SELECT trials describes the safety profile of upadacitinib, an oral Janus kinase inhibitor, for up to 5 years of exposure across psoriatic arthritis (PsA), ankylosing spondylitis (AS), and non-radiographic axial spondyloarthritis (nr-axSpA) (including pooled axial spondyloarthritis [axSpA]).
Methods: Safety data from five trials of upadacitinib in PsA (2 trials), AS (2 trials), and nr-axSpA (1 trial) were analyzed up to a data cut-off of August 15, 2022. One PsA study included adalimumab as an active comparator. Treatment-emergent adverse events (TEAEs) were summarized for PsA (pooled upadacitinib 15 mg once daily and adalimumab 40 mg biweekly), AS (pooled upadacitinib 15 mg), nr-axSpA (upadacitinib 15 mg), and pooled axSpA (pooled upadacitinib 15 mg from axSpA trials). TEAEs were reported as exposure-adjusted event rates per 100 patient-years (E/100 PY).
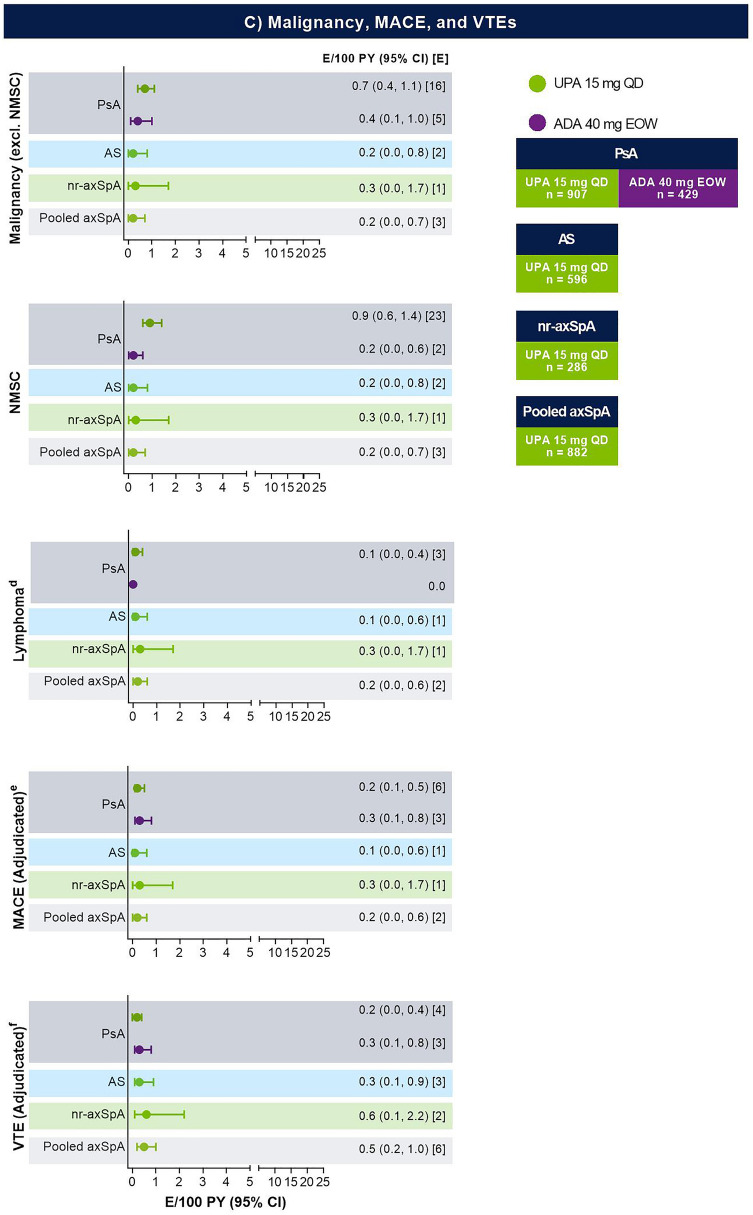
Results: A total of 1789 patients (PsA, n = 907; AS, n = 596; nr-axSpA, n = 286) received ≥ 1 dose of upadacitinib 15 mg for 3689 PY of exposure or adalimumab (n = 429) for 1147 PY of exposure. Overall TEAEs and serious TEAEs were highest in PsA and numerically higher with upadacitinib versus adalimumab; rates were similar between AS and nr-axSpA. In PsA, higher rates of serious infection, herpes zoster (HZ), lymphopenia, and nonmelanoma skin cancer (NMSC) were observed with upadacitinib versus adalimumab. Rates of malignancy excluding NMSC, adjudicated major adverse cardiovascular events, and adjudicated venous thromboembolic events were comparable between upadacitinib and adalimumab in PsA and were similar across diseases.
Conclusion: Higher rates of serious infection, HZ, lymphopenia, and NMSC were observed with upadacitinib versus adalimumab in PsA; slightly elevated rates for most of these TEAEs were seen with upadacitinib in PsA versus axSpA. Upadacitinib 15 mg demonstrated a generally consistent safety profile across disease states with no new safety signals identified.
Trial registration: SELECT-AXIS 1: NCT03178487; SELECT-AXIS 2: NCT04169373; SELECT-PsA 1: NCT03104400; SELECT-PsA 2: NCT03104374.
Keywords: Adalimumab; Ankylosing spondylitis; JAK inhibitor; Non-radiographic axial spondyloarthritis; Psoriatic arthritis; Safety; Upadacitinib.
Plain language summary
Psoriatic arthritis, ankylosing spondylitis, and non-radiographic axial spondyloarthritis are a group of diseases that cause pain and inflammation of the joints and/or spine. Safety data were combined from five studies: two in psoriatic arthritis, two in ankylosing spondylitis, and one in non-radiographic axial spondyloarthritis. Patients were treated with upadacitinib or adalimumab for up to 5 years. Adalimumab was only used for patients participating in one of the two psoriatic arthritis studies. Side effects from treatment were more common in patients with psoriatic arthritis than those with ankylosing spondylitis and non-radiographic axial spondyloarthritis; more patients with psoriatic arthritis had side effects with upadacitinib than adalimumab. A similar number of patients across treatment groups and diseases had side effects that made them stop treatment. The number of cancer cases (except cancer of the upper layer of the skin), cardiovascular issues, and blood clots were similar between the upadacitinib and adalimumab groups in psoriatic arthritis and across diseases. Serious infections, painful rashes that cause blisters (herpes zoster, also commonly referred to as shingles), low levels of white blood cells, and cancer of the upper layer of the skin were more common with upadacitinib than adalimumab in patients with psoriatic arthritis; overall, these events occurred more often with upadacitinib in patients with psoriatic arthritis than with ankylosing spondylitis and non-radiographic axial spondyloarthritis. Our results showed that the safety of upadacitinib was generally similar across diseases, and patients could tolerate it well for up to 5 years. No new safety risks were found with upadacitinib treatment.
© 2024. The Author(s).
Conflict of interest statement
Gerd R. Burmester has received honoraria for consulting and lecture from AbbVie, Janssen, Novartis, and Pfizer. Andrea Rubbert-Roth has received honoraria for lectures and consulting fees from AbbVie, Amgen, BMS, Chugai, Eli Lilly, Gilead, Janssen, Novartis, Roche, and Sanofi. Yoshiya Tanaka has received speaker fees and/or honoraria from Eli Lilly, AstraZeneca, Abbvie, Asahi Kasei, Gilead, Chugai, Boehringer-Ingelheim, GlaxoSmithKline, Eisai, Taisho, BMS, Pfizer and, Taiho; received research grants from Asahi Kasei, Mitsubishi-Tanabe, Eisai, Chugai, and Taisho. Yoshiya Tanaka is also an Editorial Board member of
Figures



References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
