

Downstream Biomarker Effects of Gantenerumab or Solanezumab in Dominantly Inherited Alzheimer Disease: The DIAN-TU-001 Randomized Clinical Trial
- PMID: 38683602
- PMCID: PMC11059071
- DOI: 10.1001/jamaneurol.2024.0991
Downstream Biomarker Effects of Gantenerumab or Solanezumab in Dominantly Inherited Alzheimer Disease: The DIAN-TU-001 Randomized Clinical Trial
Abstract
Importance: Effects of antiamyloid agents, targeting either fibrillar or soluble monomeric amyloid peptides, on downstream biomarkers in cerebrospinal fluid (CSF) and plasma are largely unknown in dominantly inherited Alzheimer disease (DIAD).
Objective: To investigate longitudinal biomarker changes of synaptic dysfunction, neuroinflammation, and neurodegeneration in individuals with DIAD who are receiving antiamyloid treatment.
Design, setting, and participants: From 2012 to 2019, the Dominantly Inherited Alzheimer Network Trial Unit (DIAN-TU-001) study, a double-blind, placebo-controlled, randomized clinical trial, investigated gantenerumab and solanezumab in DIAD. Carriers of gene variants were assigned 3:1 to either drug or placebo. The present analysis was conducted from April to June 2023. DIAN-TU-001 spans 25 study sites in 7 countries. Biofluids and neuroimaging from carriers of DIAD gene variants in the gantenerumab, solanezumab, and placebo groups were analyzed.
Interventions: In 2016, initial dosing of gantenerumab, 225 mg (subcutaneously every 4 weeks) was increased every 8 weeks up to 1200 mg. In 2017, initial dosing of solanezumab, 400 mg (intravenously every 4 weeks) was increased up to 1600 mg every 4 weeks.
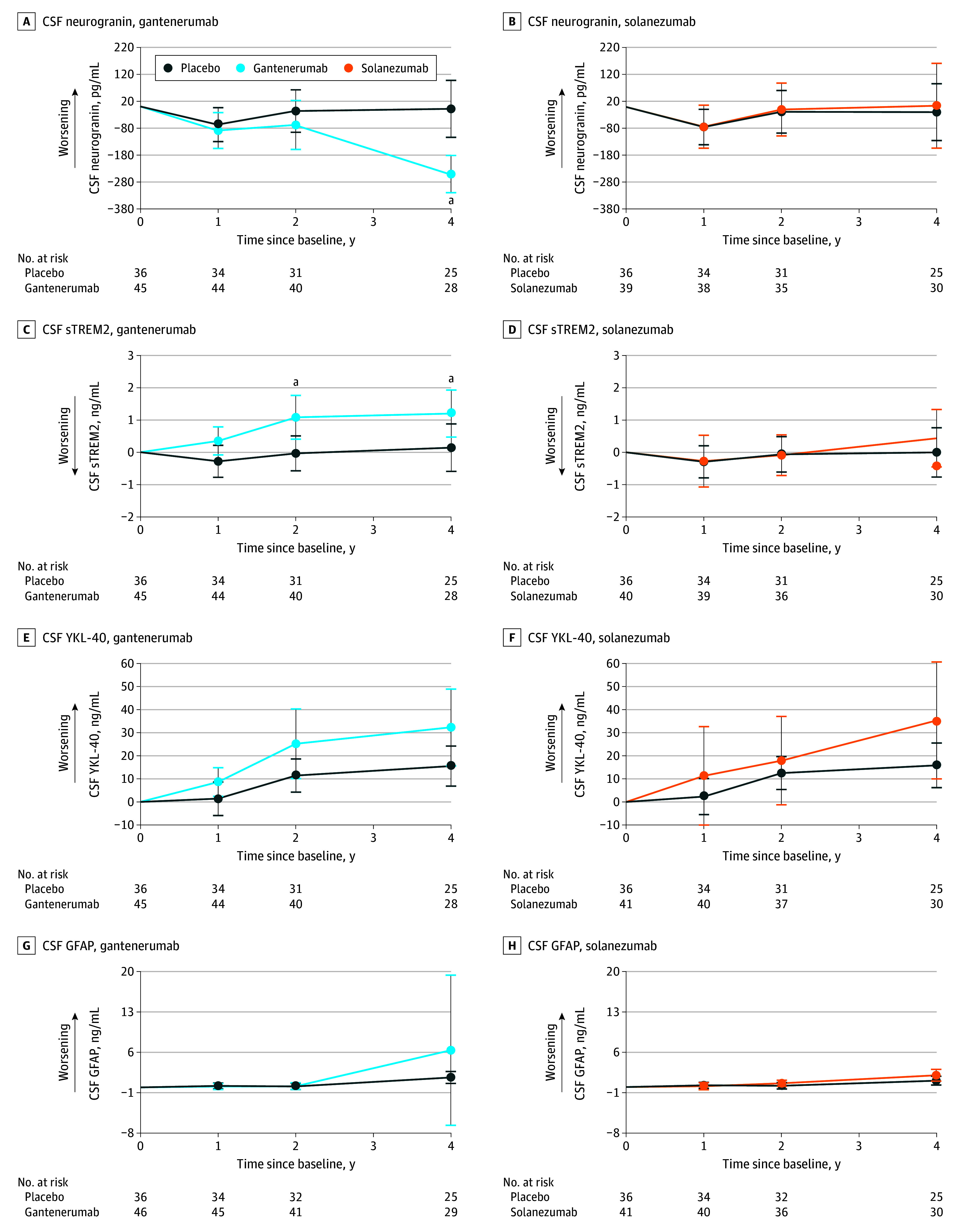
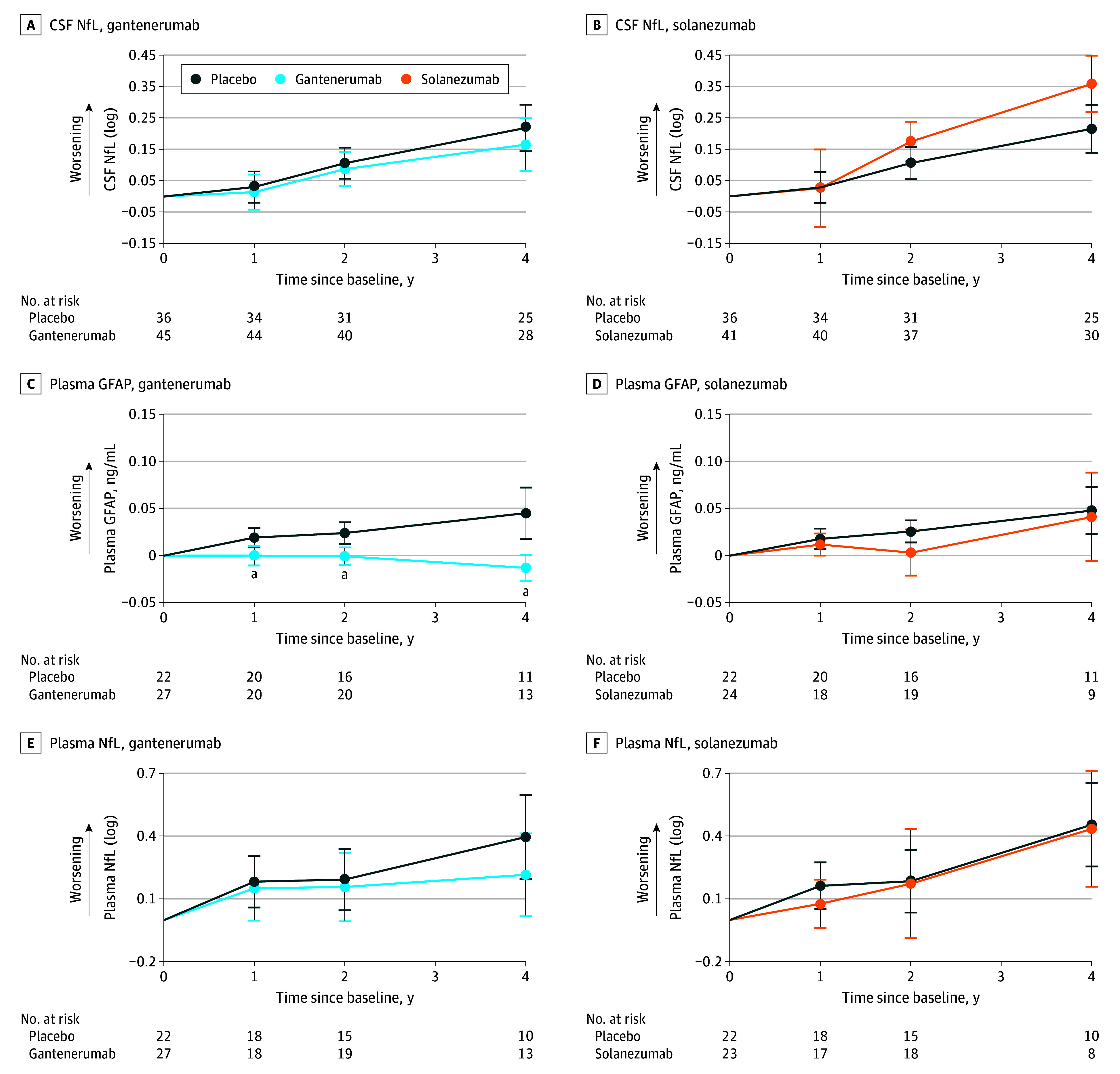
Main outcomes and measures: Longitudinal changes in CSF levels of neurogranin, soluble triggering receptor expressed on myeloid cells 2 (sTREM2), chitinase 3-like 1 protein (YKL-40), glial fibrillary acidic protein (GFAP), neurofilament light protein (NfL), and plasma levels of GFAP and NfL.
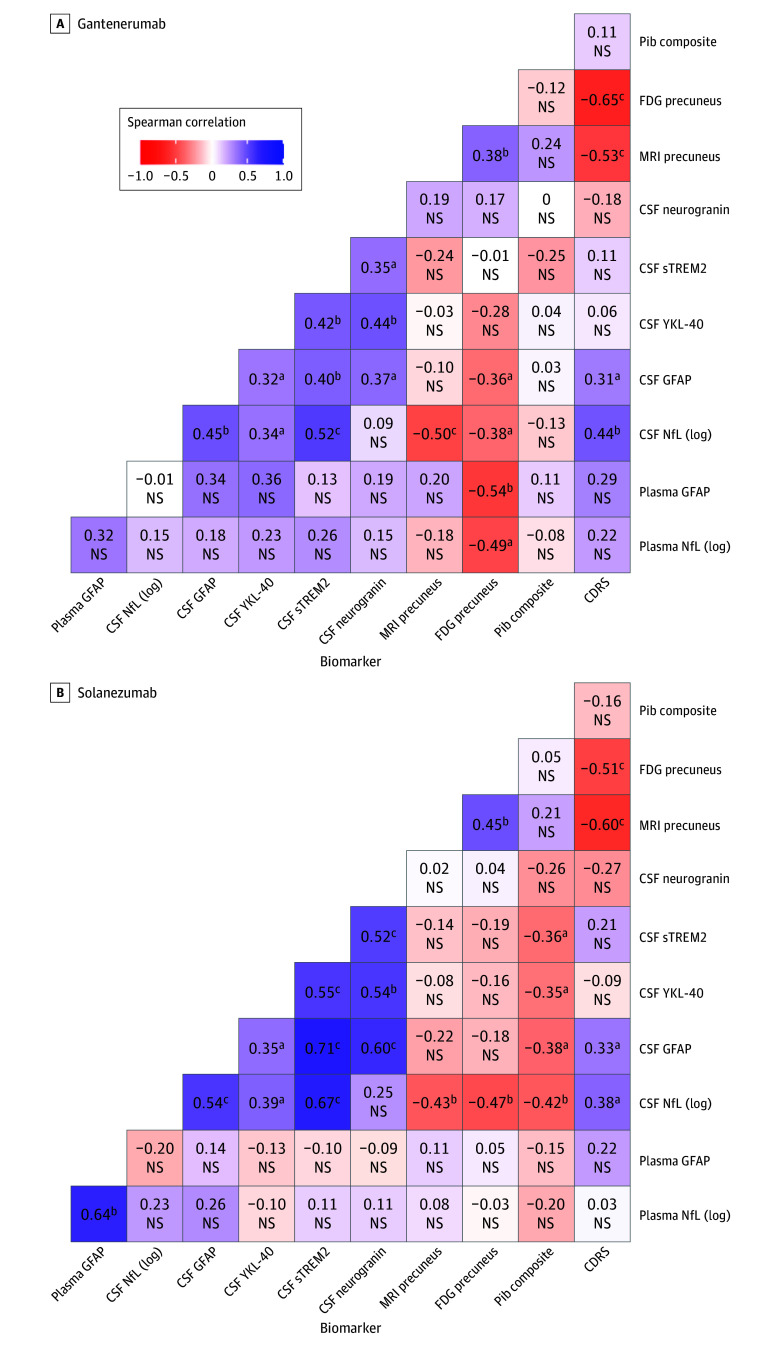
Results: Of 236 eligible participants screened, 43 were excluded. A total of 142 participants (mean [SD] age, 44 [10] years; 72 female [51%]) were included in the study (gantenerumab, 52 [37%]; solanezumab, 50 [35%]; placebo, 40 [28%]). Relative to placebo, gantenerumab significantly reduced CSF neurogranin level at year 4 (mean [SD] β = -242.43 [48.04] pg/mL; P < .001); reduced plasma GFAP level at year 1 (mean [SD] β = -0.02 [0.01] ng/mL; P = .02), year 2 (mean [SD] β = -0.03 [0.01] ng/mL; P = .002), and year 4 (mean [SD] β = -0.06 [0.02] ng/mL; P < .001); and increased CSF sTREM2 level at year 2 (mean [SD] β = 1.12 [0.43] ng/mL; P = .01) and year 4 (mean [SD] β = 1.06 [0.52] ng/mL; P = .04). Solanezumab significantly increased CSF NfL (log) at year 4 (mean [SD] β = 0.14 [0.06]; P = .02). Correlation analysis for rates of change found stronger correlations between CSF markers and fluid markers with Pittsburgh compound B positron emission tomography for solanezumab and placebo.
Conclusions and relevance: This randomized clinical trial supports the importance of fibrillar amyloid reduction in multiple AD-related processes of neuroinflammation and neurodegeneration in CSF and plasma in DIAD. Additional studies of antiaggregated amyloid therapies in sporadic AD and DIAD are needed to determine the utility of nonamyloid biomarkers in determining disease modification.
Trial registration: ClinicalTrials.gov Identifier: NCT04623242.
Conflict of interest statement
Figures
Comment on
-
Fluid Biomarker Changes After Amyloid-β-Targeting Drugs.JAMA Neurol. 2024 Jun 1;81(6):579-581. doi: 10.1001/jamaneurol.2024.1103. JAMA Neurol. 2024. PMID: 38683615 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
