

Sociodemographic Factors and Trends in Bronchiolitis-Related Emergency Department Visit and Hospitalization Rates
- PMID: 38683605
- PMCID: PMC11059049
- DOI: 10.1001/jamanetworkopen.2024.8976
Sociodemographic Factors and Trends in Bronchiolitis-Related Emergency Department Visit and Hospitalization Rates
Abstract
Importance: Bronchiolitis is the most common and most cumulatively expensive condition in pediatric hospital care. Few population-based studies have examined health inequalities in bronchiolitis outcomes over time.
Objective: To examine trends in bronchiolitis-related emergency department (ED) visit and hospitalization rates by sociodemographic factors in a universally funded health care system.
Design, setting, and participants: This repeated cross-sectional cohort study was performed from April 1, 2004, to March 31, 2022, using population-based health administrative data from children younger than 2 years in Ontario, Canada.
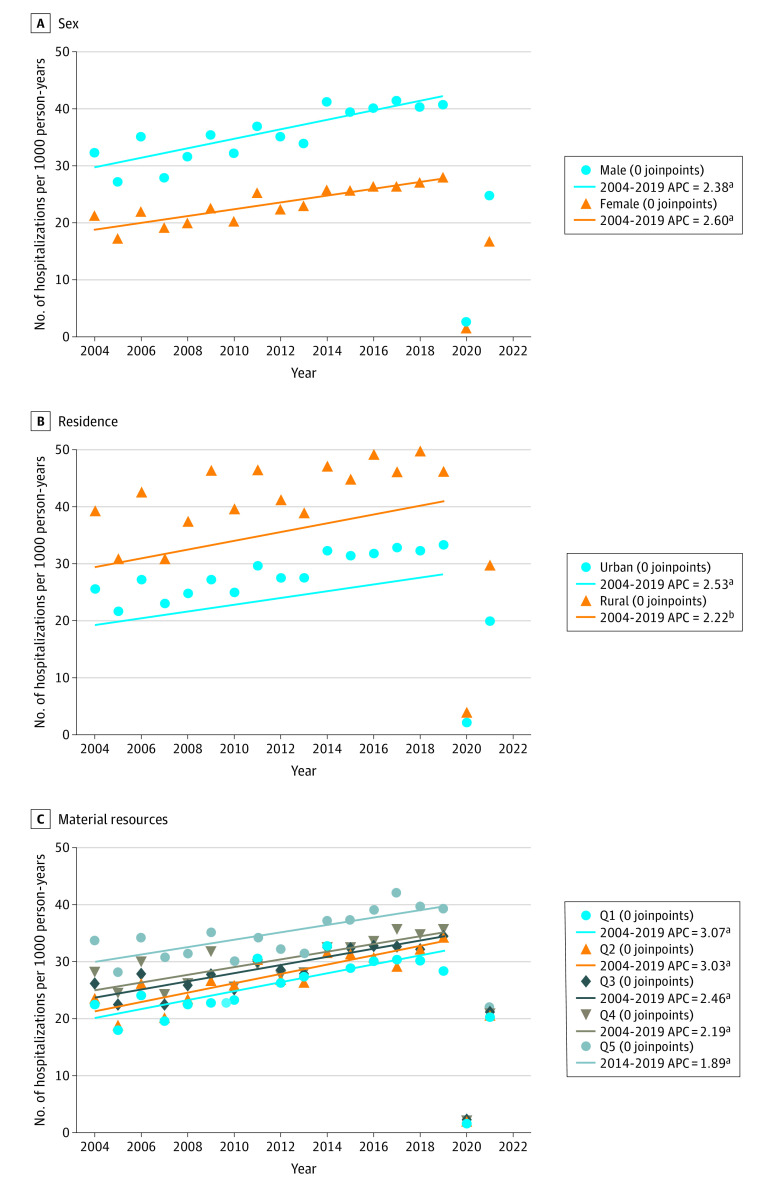
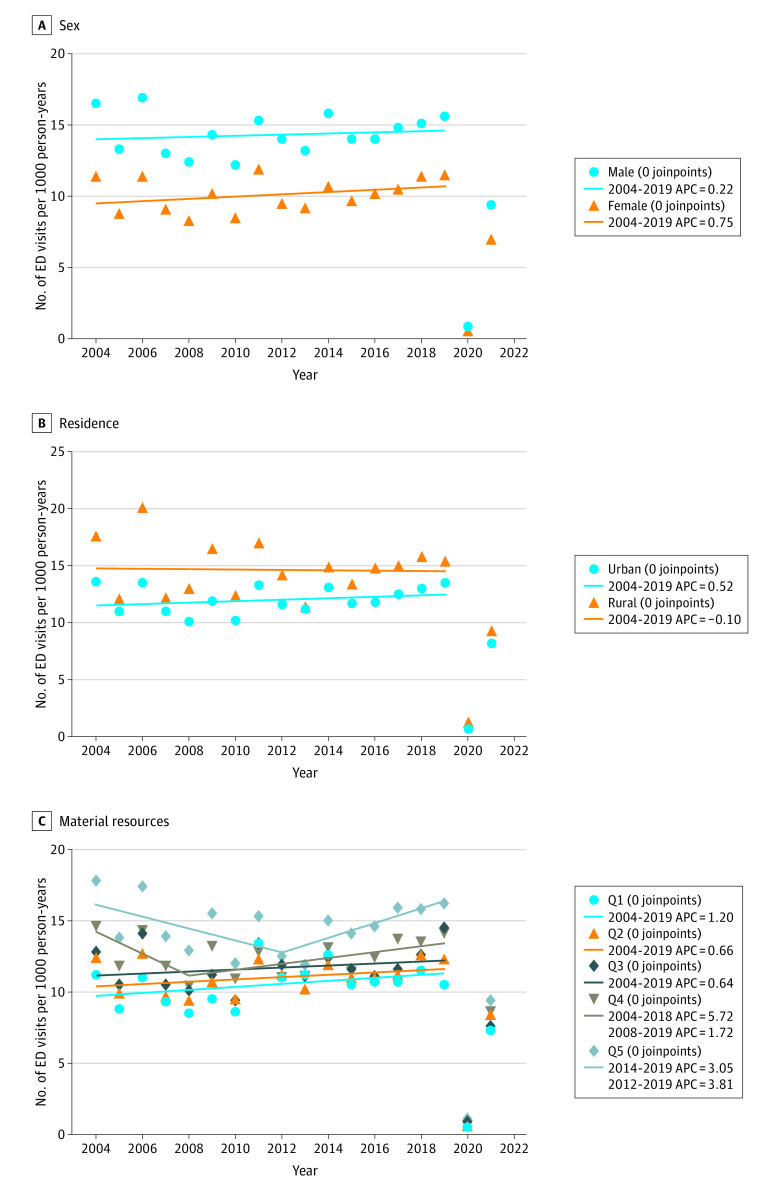
Main outcome and measures: Bronchiolitis ED visit and hospitalization rates per 1000 person-years reported for the equity stratifiers of sex, residence location (rural vs urban), and material resources quintile. Trends in annual rates by equity stratifiers were analyzed using joinpoint regression and estimating the average annual percentage change (AAPC) with 95% CI and the absolute difference in AAPC with 95% CI from April 1, 2004, to March 31, 2020.
Results: Of 2 921 573 children included in the study, 1 422 088 (48.7%) were female and 2 619 139 (89.6%) lived in an urban location. Emergency department visit and hospitalization rates were highest for boys, those with rural residence, and those with least material resources. There were no significant between-group absolute differences in the AAPC in ED visits per 1000 person-years by sex (female vs male; 0.22; 95% CI, -0.92 to 1.35; P = .71), residence (rural vs urban; -0.31; 95% CI -1.70 to 1.09; P = .67), or material resources (quintile 5 vs 1; -1.17; 95% CI, -2.57 to 0.22; P = .10). Similarly, there were no significant between-group absolute differences in the AAPC in hospitalizations per 1000 person-years by sex (female vs male; 0.53; 95% CI, -1.11 to 2.17; P = .53), residence (rural vs urban; -0.62; 95% CI, -2.63 to 1.40; P = .55), or material resources (quintile 5 vs 1; -0.93; 95% CI -3.80 to 1.93; P = .52).
Conclusions and relevance: In this population-based cohort study of children in a universally funded health care system, inequalities in bronchiolitis ED visit and hospitalization rates did not improve over time.
Conflict of interest statement
Figures
References
-
- Public Health Agency of Canada (PHAC) . Reducing Health Inequalities: A Challenge For Our Times. Accessed November 22, 2023. https://publications.gc.ca/collections/collection_2012/aspc-phac/HP35-22...
-
- World Health Organization . Health Impact Assessment, Glossary of Terms. Accessed November 18, 2023. https://www.who.int/docs/default-source/documents/publications/glossary-...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
