

Effectiveness of Blended Versus Traditional Refresher Training for Cardiopulmonary Resuscitation: Prospective Observational Study
- PMID: 38683663
- PMCID: PMC11091803
- DOI: 10.2196/52230
Effectiveness of Blended Versus Traditional Refresher Training for Cardiopulmonary Resuscitation: Prospective Observational Study
Abstract
Background: Generally, cardiopulmonary resuscitation (CPR) skills decline substantially over time. By combining web-based self-regulated learning with hands-on practice, blended training can be a time- and resource-efficient approach enabling individuals to acquire or refresh CPR skills at their convenience. However, few studies have evaluated the effectiveness of blended CPR refresher training compared with that of the traditional method.
Objective: This study investigated and compared the effectiveness of traditional and blended CPR training through 6-month and 12-month refresher sessions with CPR ability indicators.
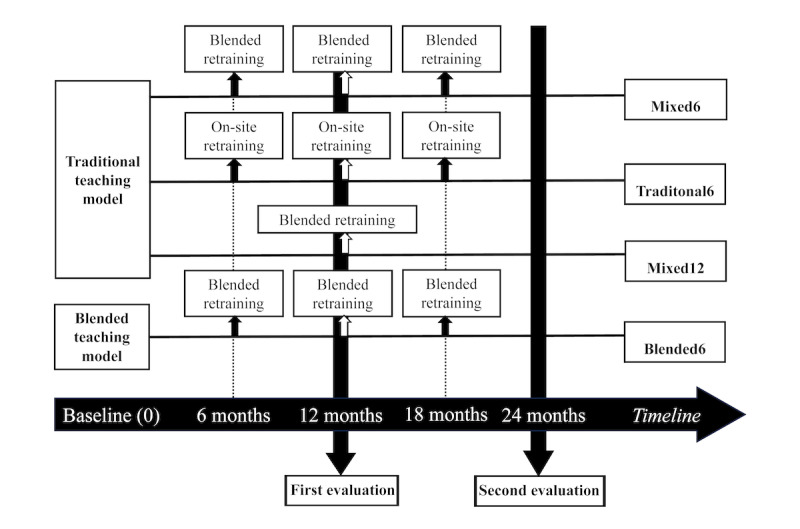
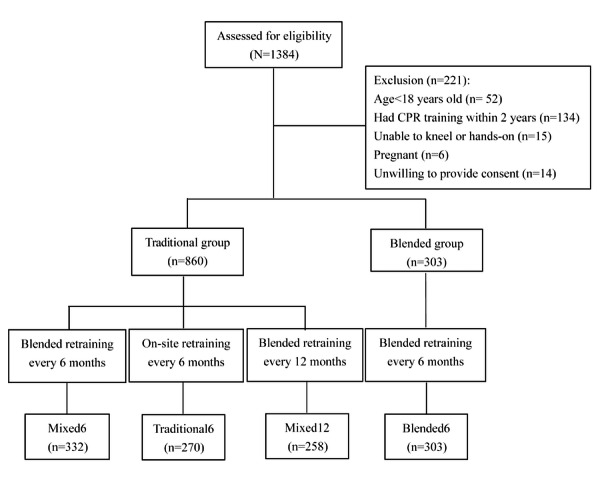
Methods: This study recruited participants aged ≥18 years from the Automated External Defibrillator Donation Project. The participants were divided into 4 groups based on the format of the CPR training and refresher training received: (1) initial traditional training (a 30-minute instructor-led, hands-on session) and 6-month traditional refresher training (Traditional6 group), (2) initial traditional training and 6-month blended refresher training (an 18-minute e-learning module; Mixed6 group), (3) initial traditional training and 12-month blended refresher training (Mixed12 group), and (4) initial blended training and 6-month blended refresher training (Blended6 group). CPR knowledge and performance were evaluated immediately after initial training. For each group, following initial training but before refresher training, a learning effectiveness assessment was conducted at 12 and 24 months. CPR knowledge was assessed using a written test with 15 multiple-choice questions, and CPR performance was assessed through an examiner-rated skill test and objectively through manikin feedback. A generalized estimating equation model was used to analyze changes in CPR ability indicators.
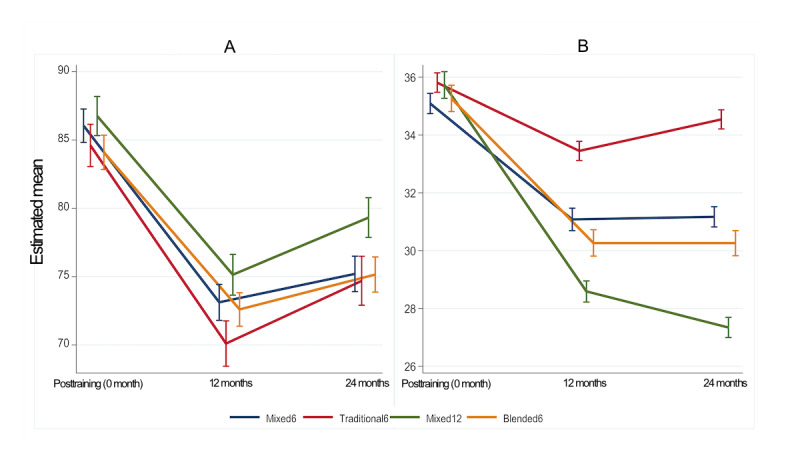
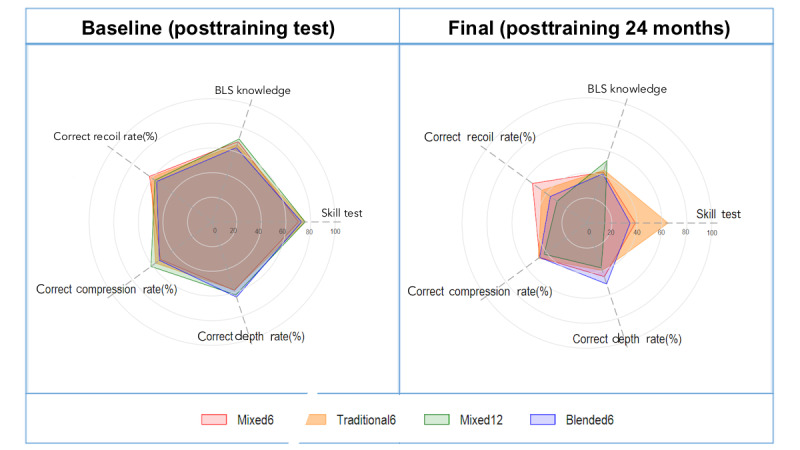
Results: This study recruited 1163 participants (mean age 41.82, SD 11.6 years; n=725, 62.3% female), with 332 (28.5%), 270 (23.2%), 258 (22.2%), and 303 (26.1%) participants in the Mixed6, Traditional6, Mixed12, and Blended6 groups, respectively. No significant between-group difference was observed in knowledge acquisition after initial training (P=.23). All groups met the criteria for high-quality CPR skills (ie, average compression depth: 5-6 cm; average compression rate: 100-120 beats/min; chest recoil rate: >80%); however, a higher proportion (98/303, 32.3%) of participants receiving blended training initially demonstrated high-quality CPR skills. At 12 and 24 months, CPR skills had declined in all the groups, but the decline was significantly higher in the Mixed12 group, whereas the differences were not significant between the other groups. This finding indicates that frequent retraining can maintain high-quality CPR skills and that blended refresher training is as effective as traditional refresher training.
Conclusions: Our findings indicate that 6-month refresher training sessions for CPR are more effective for maintaining high-quality CPR skills, and that as refreshers, self-learning e-modules are as effective as instructor-led sessions. Although the blended learning approach is cost and resource effective, factors such as participant demographics, training environment, and level of engagement must be considered to maximize the potential of this approach.
Trial registration: IGOGO NCT05659108; https://www.cgmh-igogo.tw.
Keywords: CPR; blended; blended method; cardiac; cardiopulmonary; cardiopulmonary resuscitation; continuing education; emergency; hybrid; instruction; life support; observational; professional development; refresher; refreshers; rescue; resuscitation; retraining; self-directed learning; teaching; traditional method; training.
©Cheng-Yu Chien, Shang-Li Tsai, Chien-Hsiung Huang, Ming-Fang Wang, Chi-Chun Lin, Chen-Bin Chen, Li-Heng Tsai, Hsiao-Jung Tseng, Yan-Bo Huang, Chip-Jin Ng. Originally published in JMIR Medical Education (https://mededu.jmir.org), 29.04.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
The Effectiveness of Online-Only Blended Cardiopulmonary Resuscitation Training: Static-Group Comparison Study.J Med Internet Res. 2023 Apr 5;25:e42325. doi: 10.2196/42325. J Med Internet Res. 2023. PMID: 37018023 Free PMC article.
-
Comparing the effectiveness of a group-directed video instruction versus instructor-led traditional classroom instruction for learning cardiopulmonary resuscitation skills among first-year medical students: A prospective randomized controlled study.GMS J Med Educ. 2022 Sep 15;39(4):Doc45. doi: 10.3205/zma001566. eCollection 2022. GMS J Med Educ. 2022. PMID: 36310890 Free PMC article. Clinical Trial.
-
An audiovisual feedback device for compression depth, rate and complete chest recoil can improve the CPR performance of lay persons during self-training on a manikin.Physiol Meas. 2011 Jun;32(6):687-99. doi: 10.1088/0967-3334/32/6/006. Epub 2011 May 23. Physiol Meas. 2011. PMID: 21606561
-
Associations between cardiopulmonary resuscitation (CPR) knowledge, self-efficacy, training history and willingness to perform CPR and CPR psychomotor skills: A systematic review.Resuscitation. 2019 May;138:259-272. doi: 10.1016/j.resuscitation.2019.03.019. Epub 2019 Mar 27. Resuscitation. 2019. PMID: 30928504
-
Knowledge and skill level among non-healthcare providers regarding cardiopulmonary resuscitation (CPR) training in the Middle East (Arab countries): a systematic review and meta-analysis.BMC Public Health. 2024 Aug 1;24(1):2081. doi: 10.1186/s12889-024-19575-7. BMC Public Health. 2024. PMID: 39090594 Free PMC article.
Cited by
-
Impact of Video-Based Error Correction Learning for Cardiopulmonary Resuscitation Training: Quasi-Experimental Study.JMIR Serious Games. 2024 Oct 3;12:e53577. doi: 10.2196/53577. JMIR Serious Games. 2024. PMID: 39361242 Free PMC article.
References
-
- Yan S, Gan Y, Jiang N, Wang R, Chen Y, Luo Z, Zong Q, Chen S, Lv C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care. 2020;24(1):61. doi: 10.1186/s13054-020-2773-2. https://ccforum.biomedcentral.com/articles/10.1186/s13054-020-2773-2 10.1186/s13054-020-2773-2 - DOI - DOI - PMC - PubMed
-
- Phattharapornjaroen P, Nimnuan W, Sanguanwit P, Atiksawedparit P, Phontabtim M, Mankong Y. Characteristics and outcomes of out-of-hospital cardiac arrest patients before and during the COVID-19 pandemic in Thailand. Int J Emerg Med. 2022;15(1):46. doi: 10.1186/s12245-022-00444-2. https://intjem.biomedcentral.com/articles/10.1186/s12245-022-00444-2 10.1186/s12245-022-00444-2 - DOI - DOI - PMC - PubMed
-
- Chien CY, Tsai SL, Tsai LH, Chen CB, Seak CJ, Weng YM, Lin CC, Ng CJ, Chien WC, Huang CH, Lin CY, Chaou CH, Liu PH, Tseng HJ, Fang CT. Impact of transport time and cardiac arrest centers on the neurological outcome after out-of-hospital cardiac arrest: a retrospective cohort study. J Am Heart Assoc. 2020;9(11):e015544. doi: 10.1161/JAHA.119.015544. https://www.ahajournals.org/doi/10.1161/JAHA.119.015544?url_ver=Z39.88-2... - DOI - DOI - PMC - PubMed
-
- Bunch TJ, White RD, Gersh BJ, Meverden RA, Hodge DO, Ballman KV, Hammill SC, Shen WK, Packer DL. Long-term outcomes of out-of-hospital cardiac arrest after successful early defibrillation. N Engl J Med. 2003;348(26):2626–2633. doi: 10.1056/NEJMoa023053. https://www.nejm.org/doi/full/10.1056/NEJMoa023053 348/26/2626 - DOI - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
