

Who is missed in a community-based survey: Assessment and implications of biases due to incomplete sampling frame in a community-based serosurvey, Choma and Ndola Districts, Zambia, 2022
- PMID: 38683820
- PMCID: PMC11057754
- DOI: 10.1371/journal.pgph.0003072
Who is missed in a community-based survey: Assessment and implications of biases due to incomplete sampling frame in a community-based serosurvey, Choma and Ndola Districts, Zambia, 2022
Abstract
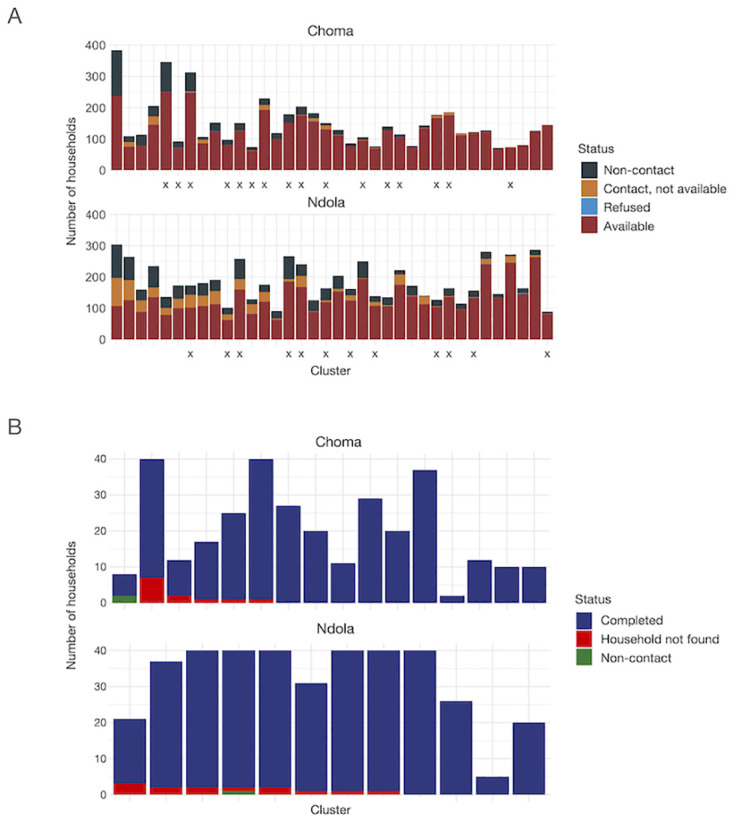
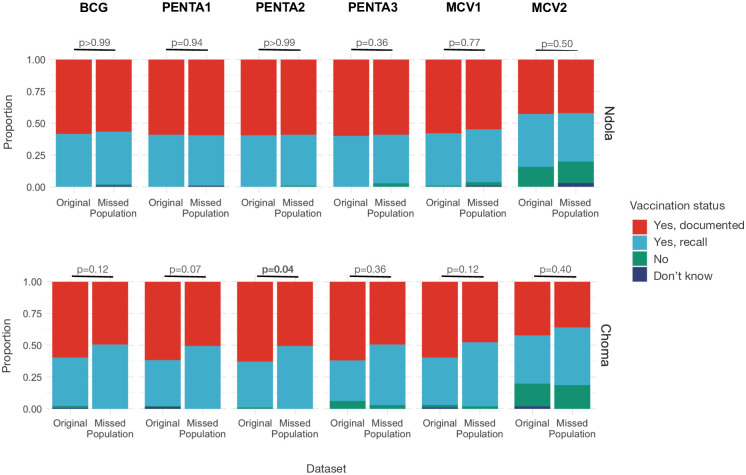
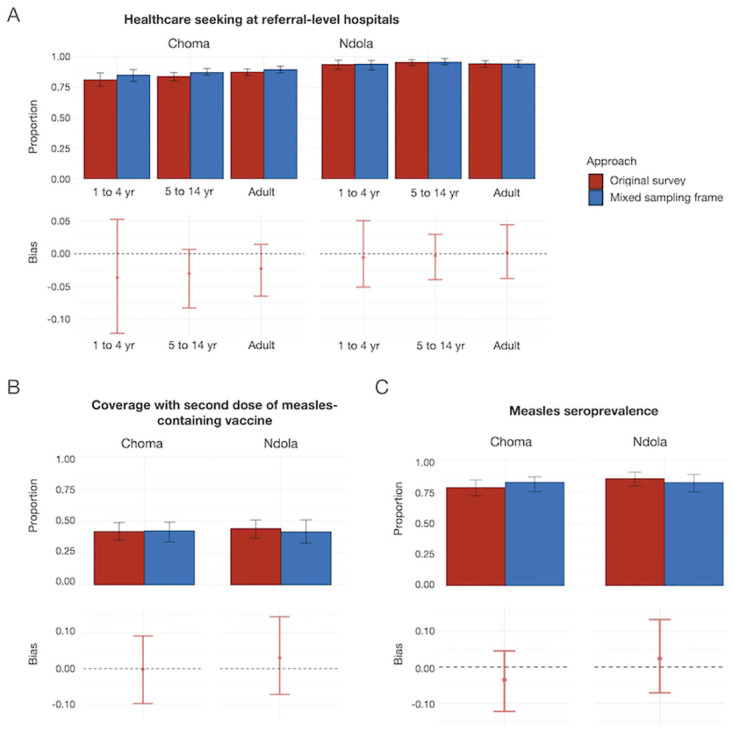
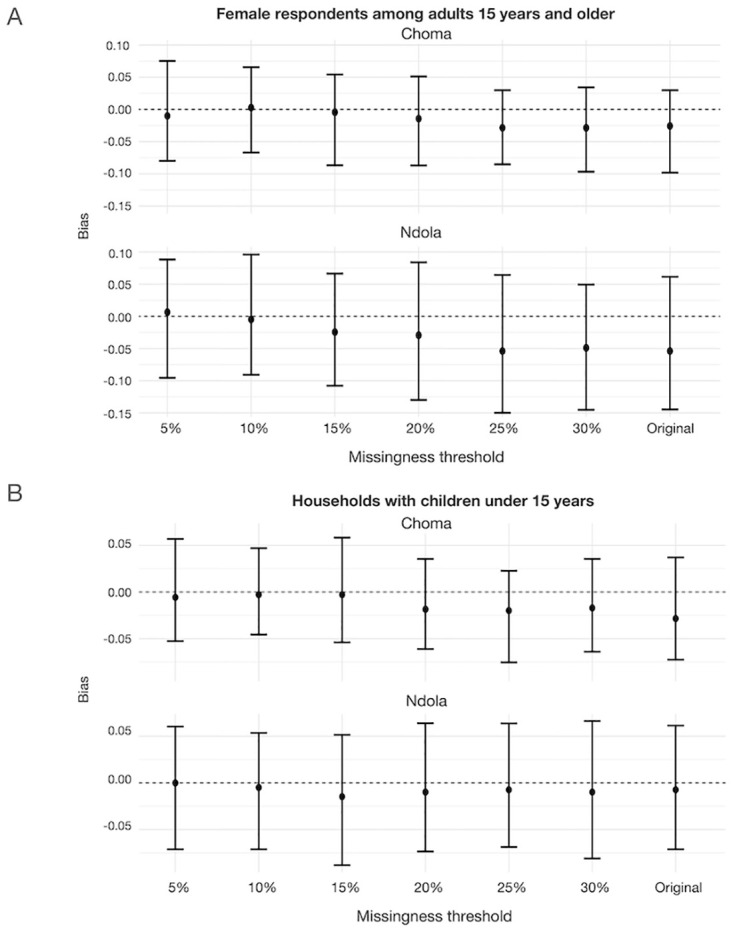
Community-based serological studies are increasingly relied upon to measure disease burden, identify population immunity gaps, and guide control and elimination strategies; however, there is little understanding of the potential for and impact of sampling biases on outcomes of interest. As part of efforts to quantify measles immunity gaps in Zambia, a community-based serological survey using stratified multi-stage cluster sampling approach was conducted in Ndola and Choma districts in May-June 2022, enrolling 1245 individuals. We carried out a follow-up study among individuals missed from the sampling frame of the serosurvey in July-August 2022, enrolling 672 individuals. We assessed the potential for and impact of biases in the community-based serosurvey by i) estimating differences in characteristics of households and individuals included and excluded (77% vs 23% of households) from the sampling frame of the serosurvey and ii) evaluating the magnitude these differences make on healthcare-seeking behavior, vaccination coverage, and measles seroprevalence. We found that missed households were 20% smaller and 25% less likely to have children. Missed individuals resided in less wealthy households, had different distributions of sex and occupation, and were more likely to seek care at health facilities. Despite these differences, simulating a survey in which missed households were included in the sampling frame resulted in less than a 5% estimated bias in these outcomes. Although community-based studies are upheld as the gold standard study design in assessing immunity gaps and underlying community health characteristics, these findings underscore the fact that sampling biases can impact the results of even well-conducted community-based surveys. Results from these studies should be interpreted in the context of the study methodology and challenges faced during implementation, which include shortcomings in establishing accurate and up-to-date sampling frames. Failure to account for these shortcomings may result in biased estimates and detrimental effects on decision-making.
Copyright: © 2024 Kostandova et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Measles and rubella serosurvey identifies rubella immunity gap in young adults of childbearing age in Zambia: The added value of nesting a serological survey within a post-campaign coverage evaluation survey.Vaccine. 2019 Apr 17;37(17):2387-2393. doi: 10.1016/j.vaccine.2019.02.037. Epub 2019 Mar 21. Vaccine. 2019. PMID: 30905529 Free PMC article.
-
How much does it cost to measure immunity? A costing analysis of a measles and rubella serosurvey in southern Zambia.PLoS One. 2020 Oct 15;15(10):e0240734. doi: 10.1371/journal.pone.0240734. eCollection 2020. PLoS One. 2020. PMID: 33057405 Free PMC article.
-
Integrating Blood Collection within Household Surveys: Lessons Learned from Nesting a Measles and Rubella Serological Survey within a Post-Campaign Coverage Evaluation Survey in Southern Province, Zambia.Am J Trop Med Hyg. 2018 Dec;99(6):1639-1642. doi: 10.4269/ajtmh.18-0320. Am J Trop Med Hyg. 2018. PMID: 30277204 Free PMC article.
-
Measuring coverage in MNCH: design, implementation, and interpretation challenges associated with tracking vaccination coverage using household surveys.PLoS Med. 2013;10(5):e1001404. doi: 10.1371/journal.pmed.1001404. Epub 2013 May 7. PLoS Med. 2013. PMID: 23667334 Free PMC article. Review.
-
Impact of summer programmes on the outcomes of disadvantaged or 'at risk' young people: A systematic review.Campbell Syst Rev. 2024 Jun 13;20(2):e1406. doi: 10.1002/cl2.1406. eCollection 2024 Jun. Campbell Syst Rev. 2024. PMID: 38873396 Free PMC article. Review.
References
-
- Rostami A, Sepidarkish M, Leeflang MMG, Riahi SM, Nourollahpour Shiadeh M, Esfandyari S, et al.. SARS-CoV-2 seroprevalence worldwide: a systematic review and meta-analysis. Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis. 2021;27: 331–340. doi: 10.1016/j.cmi.2020.10.020 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials