

Clonal hematopoiesis-derived therapy-related myeloid neoplasms after autologous hematopoietic stem cell transplant for lymphoid and non-lymphoid disorders
- PMID: 38684821
- PMCID: PMC11147764
- DOI: 10.1038/s41375-024-02258-y
Clonal hematopoiesis-derived therapy-related myeloid neoplasms after autologous hematopoietic stem cell transplant for lymphoid and non-lymphoid disorders
Abstract
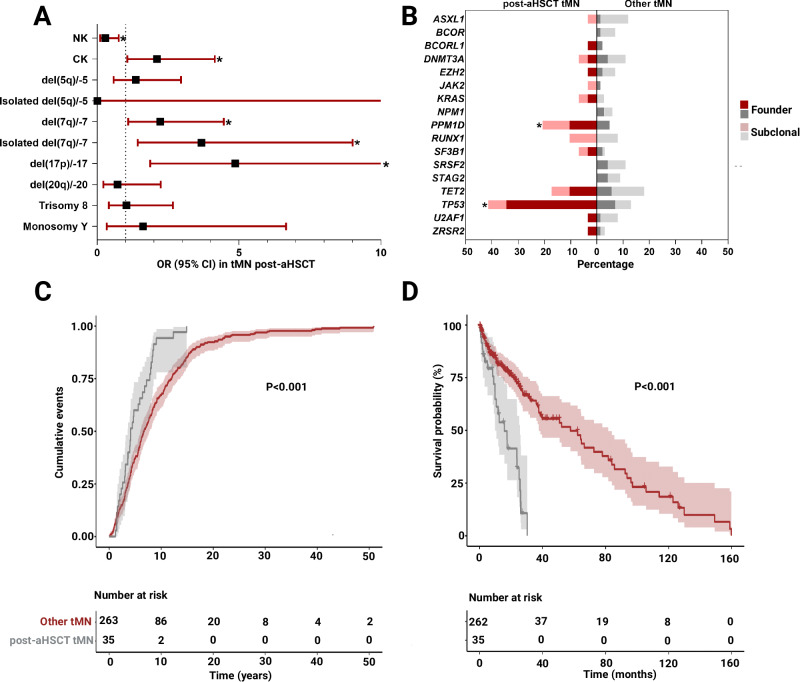
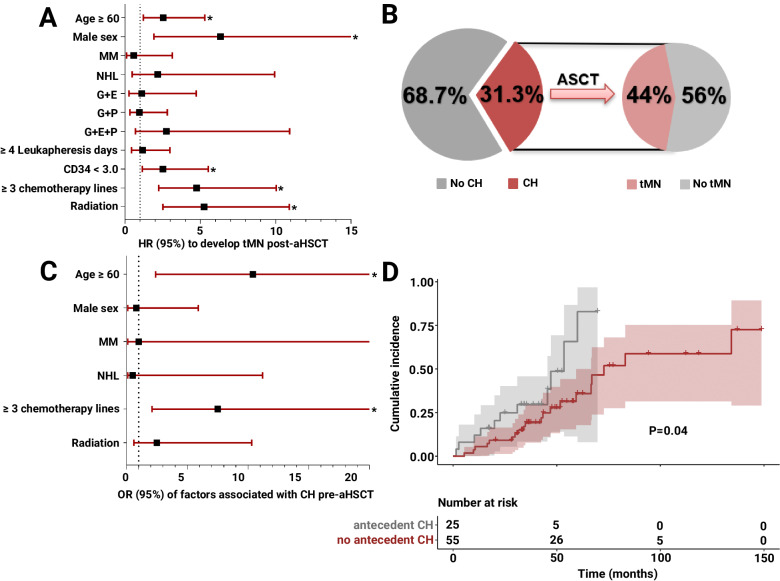
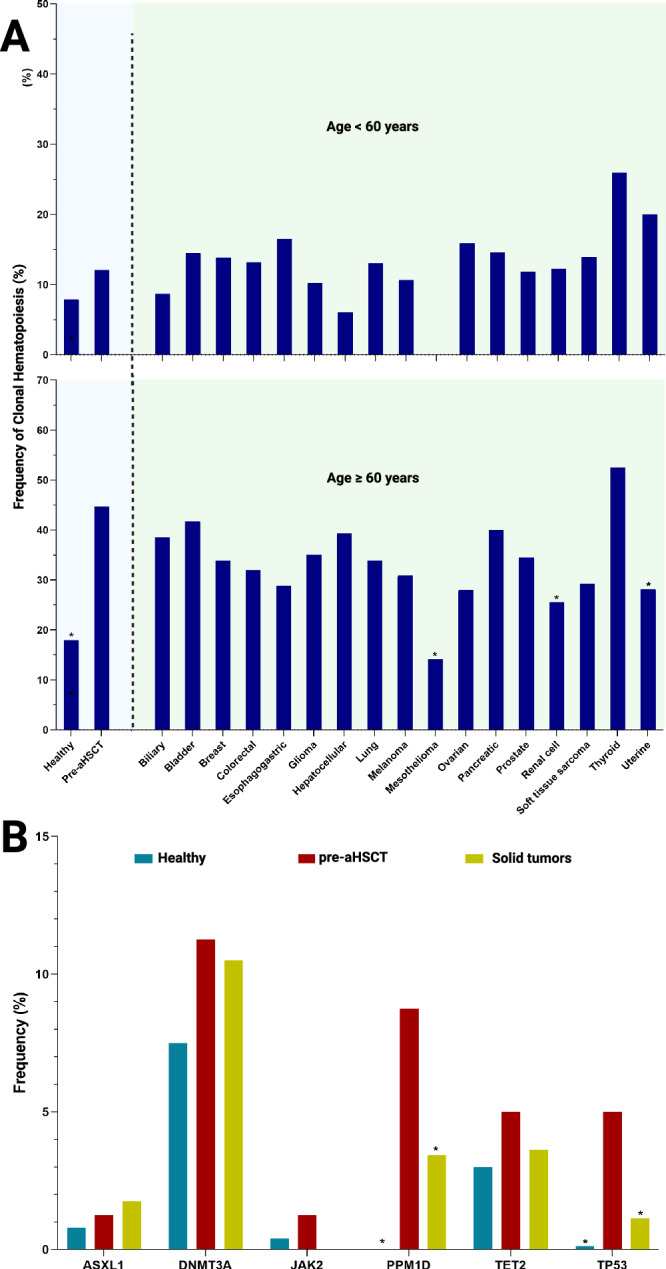
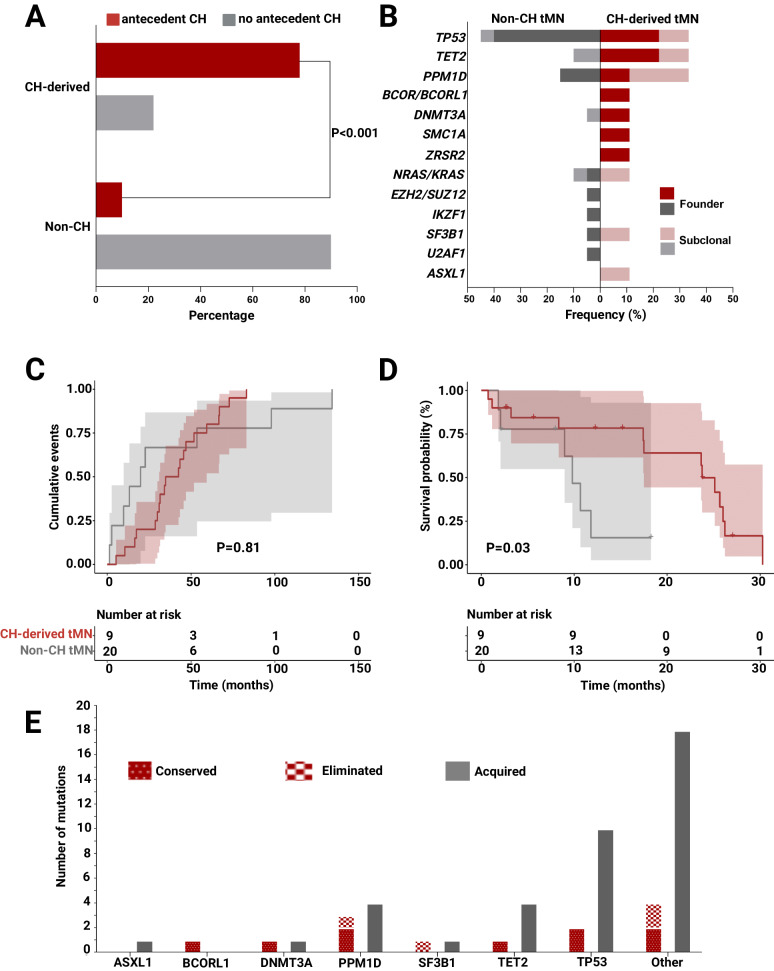
Therapy-related myeloid neoplasms (tMN) are complications of cytotoxic therapies. Risk of tMN is high in recipients of autologous hematopoietic stem cell transplantation (aHSCT). Acquisition of genomic mutations represents a key pathogenic driver but the origins, timing and dynamics, particularly in the context of preexisting or emergent clonal hematopoiesis (CH), have not been sufficiently clarified. We studied a cohort of 1507 patients undergoing aHSCT and a cohort of 263 patients who developed tMN without aHSCT to determine clinico-molecular features unique to post-aHSCT tMN. We show that tMN occurs in up to 2.3% of patients at median of 2.6 years post-AHSCT. Age ≥ 60 years, male sex, radiotherapy, high treatment burden ( ≥ 3 lines of chemotherapy), and graft cellularity increased the risk of tMN. Time to evolution and overall survival were shorter in post-aHSCT tMN vs. other tMN, and the earlier group's mutational pattern was enriched in PPM1D and TP53 lesions. Preexisting CH increased the risk of adverse outcomes including post-aHSCT tMN. Particularly, antecedent lesions affecting PPM1D and TP53 predicted tMN evolution post-transplant. Notably, CH-derived tMN had worse outcomes than non CH-derived tMN. As such, screening for CH before aHSCT may inform individual patients' prognostic outcomes and influence their prospective treatment plans. Presented in part as an oral abstract at the 2022 American Society of Hematology Annual Meeting, New Orleans, LA, 2022.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
