

Glycemic control and clinical outcomes in diabetic patients with heart failure and reduced ejection fraction: insight from ventricular remodeling using cardiac MRI
- PMID: 38685007
- PMCID: PMC11059653
- DOI: 10.1186/s12933-024-02243-w
Glycemic control and clinical outcomes in diabetic patients with heart failure and reduced ejection fraction: insight from ventricular remodeling using cardiac MRI
Abstract
Background: Glycemic control, as measured by glycosylated hemoglobin (HbA1c), is an important biomarker to evaluate diabetes severity and is believed to be associated with heart failure development. Type 2 diabetes mellitus (T2DM) and heart failure with reduced ejection fraction (HFrEF) commonly coexist, and the combination of these two diseases indicates a considerably poorer outcome than either disease alone. Therefore, glycemic control should be carefully managed. The present study aimed to explore the association between glycemic control and clinical outcomes, and to determine the optimal glycemic target in this specific population.
Methods: A total of 262 patients who underwent cardiac MRI were included and were split by HbA1c levels [HbA1c < 6.5% (intensive control), HbA1c 6.5-7.5% (modest control), and HbA1c > 7.5% (poor control)]. The biventricular volume and function, as well as left ventricular (LV) systolic strains in patients in different HbA1c categories, were measured and compared. The primary and secondary outcomes were recorded. The association of different HbA1c levels with adverse outcomes was assessed.
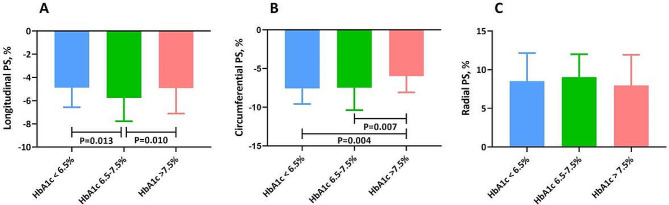
Results: Despite similar biventricular ejection fractions, both patients with intensive and poor glycemic control exhibited prominent deterioration of LV systolic strain in the longitudinal component (P = 0.004). After a median follow-up of 35.0 months, 55 patients (21.0%) experienced at least one confirmed endpoint event. Cox multivariable analysis indicated that both patients in the lowest and highest HbA1c categories exhibited a more than 2-fold increase in the risk for primary outcomes [HbA1c < 6.5%: hazard ratio (HR) = 2.42, 95% confidence interval (CI) = 1.07-5.45; P = 0.033; HbA1c > 7.5%: HR = 2.24, 95% CI = 1.01-4.99; P = 0.038] and secondary outcomes (HbA1c < 6.5%: HR = 2.84, 95% CI = 1.16-6.96; P = 0.022; HbA1c > 7.5%: HR = 2.65, 95% CI = 1.08-6.50; P = 0.038) compared with those in the middle HbA1c category.
Conclusions: We showed a U-shaped association of glycemic control with clinical outcomes in patients with T2DM and HFrEF, with the lowest risk of adverse outcomes among patients with modest glycemic control. HbA1c between 6.5% and 7.5% may be served as the optimal hypoglycemic target in this specific population.
Keywords: Glycosylated hemoglobin; Heart failure with reduced ejection fraction; Myocardial contractile dysfunction; Outcomes; Type 2 diabetes mellitus.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Lawson CA, Jones PW, Teece L, et al. Association between type 2 diabetes and all-cause hospitalization and mortality in the UK general heart failure population: stratification by diabetic glycemic control and medication intensification. JACC Heart Fail. 2018;6(1):18–26. doi: 10.1016/j.jchf.2017.08.020. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
