

Urethral-sparing laparoscopic simple prostatectomy for the treatment of benign prostatic hyperplasia with asymptomatic urethral stricture after urethral stricture surgery
- PMID: 38685008
- PMCID: PMC11059642
- DOI: 10.1186/s12894-024-01487-8
Urethral-sparing laparoscopic simple prostatectomy for the treatment of benign prostatic hyperplasia with asymptomatic urethral stricture after urethral stricture surgery
Abstract
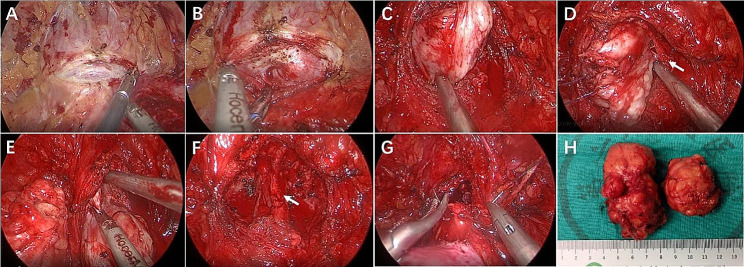
Objective: To evaluate the efficacy of urethral-sparing laparoscopic simple prostatectomy (US-LSP) for the treatment of large-volume (>80 ml) benign prostatic hyperplasia (BPH) with asymptomatic urethral stricture (urethral lumen > 16 Fr) after urethral stricture surgery.
Methods: We retrospectively analyzed clinical data of 39 large-volume BPH patients with asymptomatic urethral stricture after urethral stricture surgery who underwent US-LSP from January 2016 to October 2021. Postoperative follow-ups were scheduled at 1, 3, and 6 months.
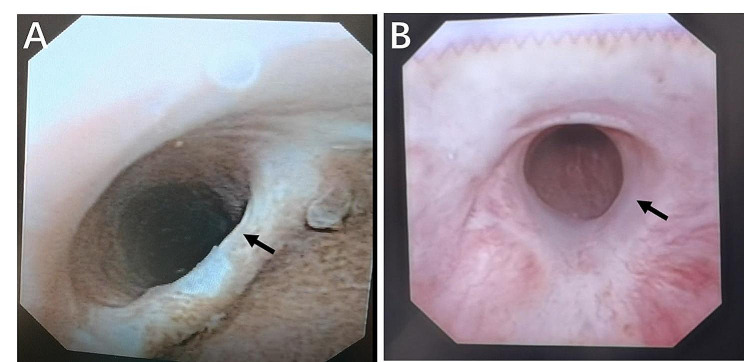
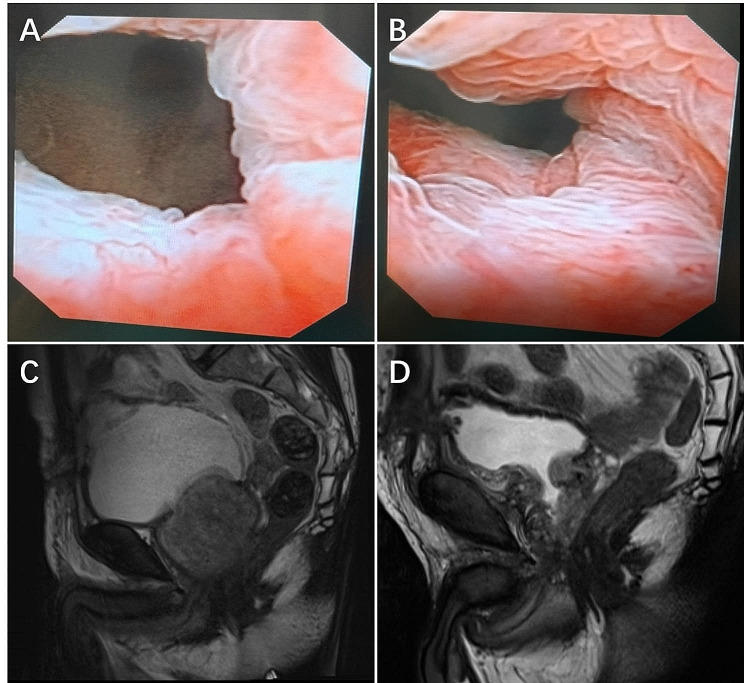
Results: All patients affected by significant BPH-related lower urinary tract symptoms (LUTS) including 22 cases with asymptomatic anterior urethral stricture and 17 cases with asymptomatic posterior urethral stricture. Median operative time was 118 min (interquartile range [IQR]100-145). Median estimated blood loss was 224 ml (IQR: 190-255). 33 patients(84.6%) avoided continuous bladder irrigation. Postoperative complications occurred in 5 patients (12.8%), including 4 cases with Clavien-Dindo grade 1 and grade 2 and 1 case with grade 3a. During follow-up, US-LSP presented statistically significant improvements in LUTS compared to baseline (P < 0.05). A total of 25 patients had normal ejaculation preoperatively and 3 patients (12%) complained retrograde ejaculation postoperatively. Two patients (5.1%) reported stress urinary incontinence (SUI) and no patient reported aggravated urethral stricture during follow-up.
Conclusions: US-LSP was safe and effective in treating large-volume BPH with asymptomatic urethral stricture after urethral stricture surgery. Meanwhile, US-LSP could reduce the risk of SUI in patients with asymptomatic posterior urethral stricture and maintain ejaculatory function in a high percentage of patients.
Keywords: Begin prostatic hyperplasia; Laparoscopy Prostatectomy; Urethral stricture.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Urethra and Ejaculation Preserving Robot-assisted Simple Prostatectomy: Near-infrared Fluorescence Imaging-guided Madigan Technique.Eur Urol. 2019 Mar;75(3):492-497. doi: 10.1016/j.eururo.2018.11.051. Epub 2018 Dec 12. Eur Urol. 2019. PMID: 30553615
-
Urethral-sparing Robot-assisted Simple Prostatectomy: An Innovative Technique to Preserve Ejaculatory Function Overcoming the Limitation of the Standard Millin Approach.Eur Urol. 2021 Aug;80(2):222-233. doi: 10.1016/j.eururo.2020.09.028. Epub 2020 Oct 5. Eur Urol. 2021. PMID: 33032850
-
Extraperitoneal laparoscopic simple prostatectomy with urethra preservation using urethral initiation as the entry point: a practical approach for the treatment of benign prostatic obstruction.World J Urol. 2022 Apr;40(4):973-982. doi: 10.1007/s00345-022-03932-5. Epub 2022 Jan 22. World J Urol. 2022. PMID: 35064801
-
Urethra-sparing minimally invasive simple prostatectomy: an old technique revisited.Curr Opin Urol. 2021 Jan;31(1):18-23. doi: 10.1097/MOU.0000000000000836. Curr Opin Urol. 2021. PMID: 33229863 Review.
-
[Management of male posterior urethral stenosis following trauma and prostatic treatments, techniques and results].Fr J Urol. 2024 Nov;34(11):102716. doi: 10.1016/j.fjurol.2024.102716. Fr J Urol. 2024. PMID: 39586656 Review. French.
References
-
- Mishra K, Baeza C, Bukavina L, Gómez RG. Modified transurethral resection of the prostate for the management of BPH-related refractory lower urinary tract symptoms in patients with a history of pelvic fracture urethral injury reconstruction. Int Urol Nephrol. 2019;51(12):2137–41. doi: 10.1007/s11255-019-02276-1. - DOI - PubMed
-
- Lumen N, Campos-Juanatey F, Dimitropoulos K, Greenwell T, Martins FE, Osman N et al. EAU Guidelines on Urethral Strictures. 2023. https://uroweb.org/guidelines/urethral-strictures.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
