

Efficacy of PE-PLIF with a novel ULBD approach for lumbar degeneration diseases: a large-channel endoscopic retrospective study
- PMID: 38685055
- PMCID: PMC11057128
- DOI: 10.1186/s13018-024-04755-3
Efficacy of PE-PLIF with a novel ULBD approach for lumbar degeneration diseases: a large-channel endoscopic retrospective study
Abstract
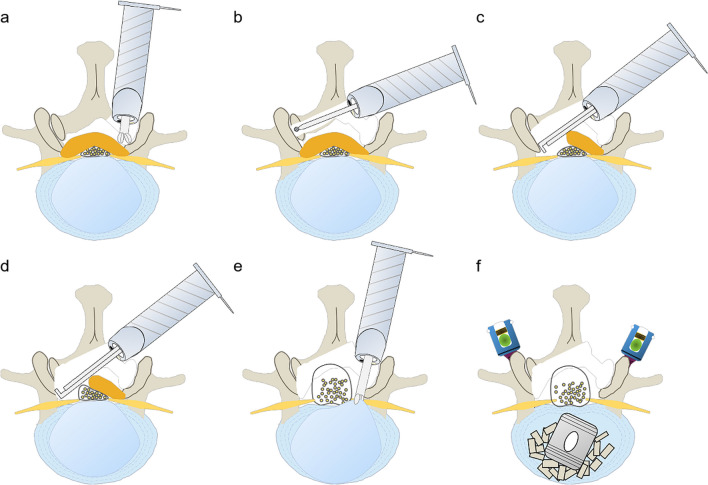
Purpose: This study aims to assess the effectiveness of Percutaneous Endoscopic Posterior Lumbar Interbody Fusion (PE-PLIF) combined with a novel Unilateral Laminotomy for Bilateral Decompression (ULBD) approach using a large-channel endoscope in treating Lumbar Degenerative Diseases (LDD).
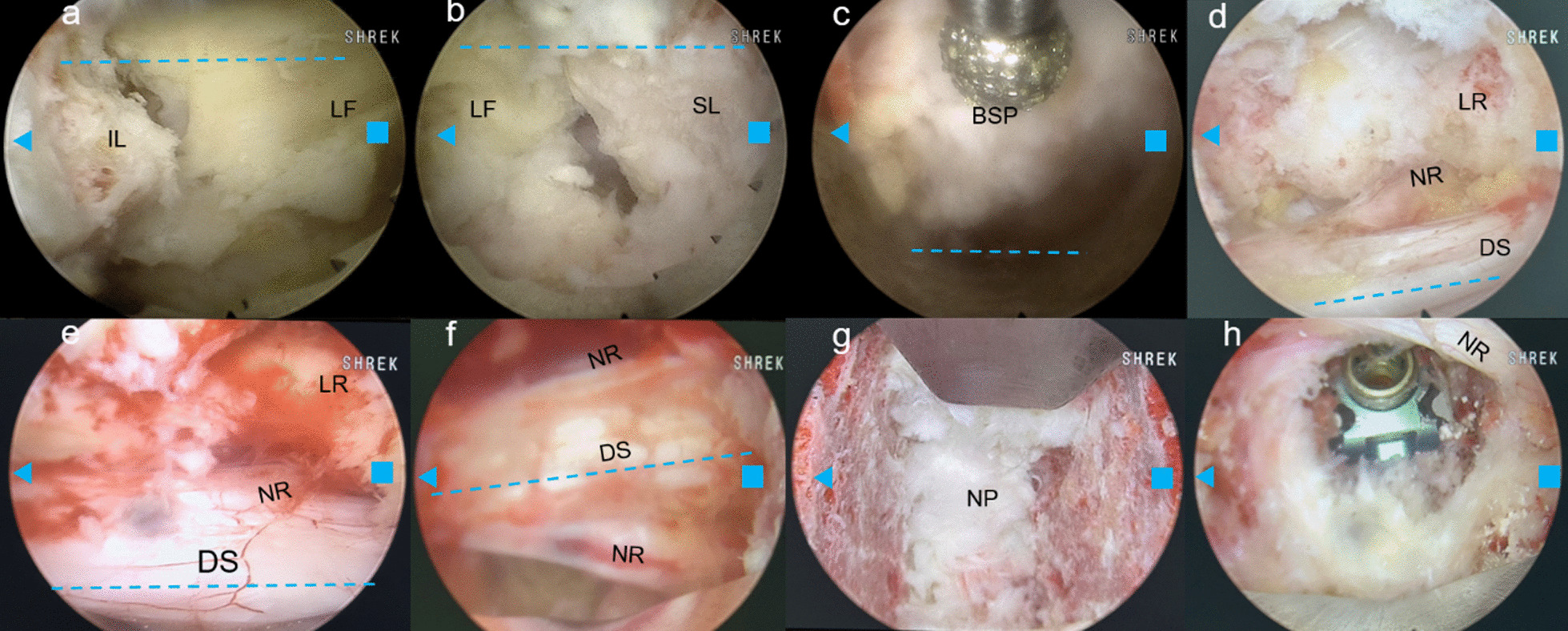
Methods: This retrospective analysis evaluates 41 LDD patients treated with PE-PLIF and ULBD from January 2021 to June 2023. A novel ULBD approach, called 'Non-touch Over-Top' technique, was utilized in this study. We compared preoperative and postoperative metrics such as demographic data, Visual Analogue Scale (VAS) for pain, Oswestry Disability Index (ODI), Japanese Orthopedic Association (JOA) score, surgical details, and radiographic changes.
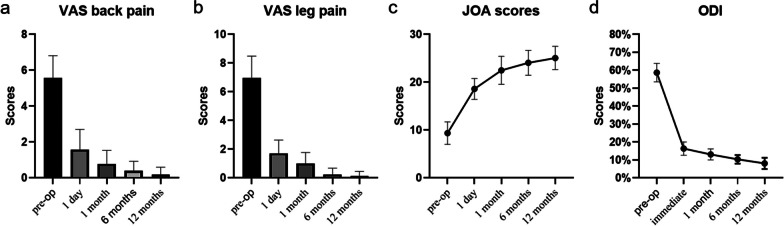
Results: The average follow-up duration was 14.41 ± 2.86 months. Notable improvements were observed postoperatively in VAS scores for back and leg pain (from 5.56 ± 0.20 and 6.95 ± 0.24 to 0.20 ± 0.06 and 0.12 ± 0.05), ODI (from 58.68 ± 0.80% to 8.10 ± 0.49%), and JOA scores (from 9.37 ± 0.37 to 25.07 ± 0.38). Radiographic measurements showed significant improvements in lumbar and segmental lordosis angles, disc height, and spinal canal area. A high fusion rate (97.56% at 6 months, 100% at 12 months) and a low cage subsidence rate (2.44%) were noted.
Conclusions: PE-PLIF combined with the novel ULBD technique via a large-channel endoscope offers significant short-term benefits for LDD management. The procedure effectively expands spinal canal volume, decompresses nerve structures, improves lumbar alignment, and stabilizes the spine. Notably, it improves patients' quality of life and minimizes complications, highlighting its potential as a promising LDD treatment option.
Keywords: Large-channel endoscope; Non-touch over-Top technique; PE-PLIF; ULBD.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Comparison of Endoscopic Unilateral Laminectomy for Bilateral Decompression (Endo-ULBD) and Posterior Lumbar Interbody Fusion (PLIF) in Managing Multi-Segmental Lumbar Spinal Stenosis: Technique and Early Outcomes.Orthop Surg. 2025 Jun;17(6):1620-1632. doi: 10.1111/os.70013. Epub 2025 Apr 23. Orthop Surg. 2025. PMID: 40269503 Free PMC article.
-
Percutaneous Endoscopic Unilateral Laminotomy and Bilateral Decompression for Lumbar Spinal Stenosis.Orthop Surg. 2021 Apr;13(2):641-650. doi: 10.1111/os.12925. Epub 2021 Feb 9. Orthop Surg. 2021. PMID: 33565271 Free PMC article.
-
Percutaneous Endoscopic Posterior Lumbar Interbody Fusion with Unilateral Laminotomy for Bilateral Decompression Vs. Open Posterior Lumbar Interbody Fusion for the Treatment of Lumbar Spondylolisthesis.Front Surg. 2022 May 25;9:915522. doi: 10.3389/fsurg.2022.915522. eCollection 2022. Front Surg. 2022. PMID: 35693306 Free PMC article.
-
Unilateral versus bilateral pedicle screw fixation with posterior lumbar interbody fusion for lumbar degenerative diseases: A meta-analysis.Medicine (Baltimore). 2017 May;96(21):e6882. doi: 10.1097/MD.0000000000006882. Medicine (Baltimore). 2017. PMID: 28538379 Free PMC article. Review.
-
Dynamic Stabilization Adjacent to Fusion versus Posterior Lumbar Interbody Fusion for the Treatment of Lumbar Degenerative Disease: A Meta-Analysis.Biomed Res Int. 2020 May 20;2020:9309134. doi: 10.1155/2020/9309134. eCollection 2020. Biomed Res Int. 2020. PMID: 32550234 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
