

Critical assessment of variant prioritization methods for rare disease diagnosis within the rare genomes project
- PMID: 38685113
- PMCID: PMC11057178
- DOI: 10.1186/s40246-024-00604-w
Critical assessment of variant prioritization methods for rare disease diagnosis within the rare genomes project
Abstract
Background: A major obstacle faced by families with rare diseases is obtaining a genetic diagnosis. The average "diagnostic odyssey" lasts over five years and causal variants are identified in under 50%, even when capturing variants genome-wide. To aid in the interpretation and prioritization of the vast number of variants detected, computational methods are proliferating. Knowing which tools are most effective remains unclear. To evaluate the performance of computational methods, and to encourage innovation in method development, we designed a Critical Assessment of Genome Interpretation (CAGI) community challenge to place variant prioritization models head-to-head in a real-life clinical diagnostic setting.
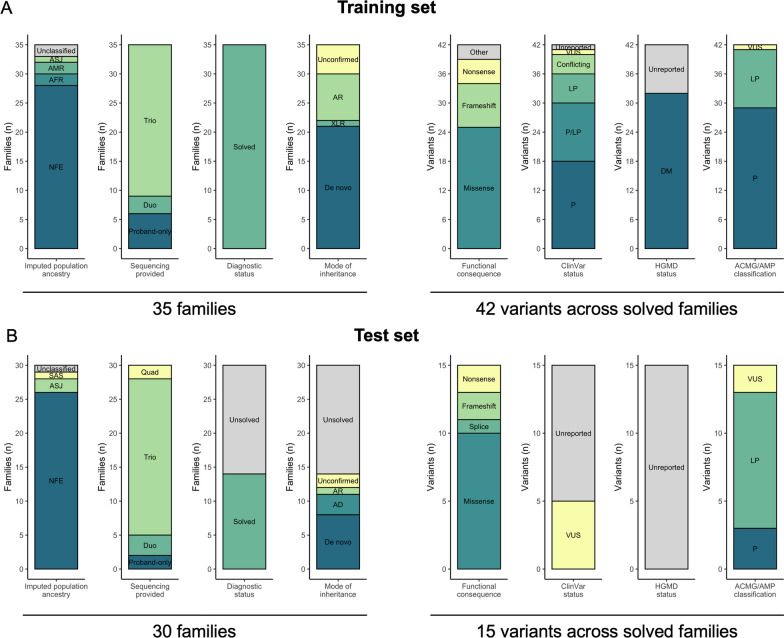
Methods: We utilized genome sequencing (GS) data from families sequenced in the Rare Genomes Project (RGP), a direct-to-participant research study on the utility of GS for rare disease diagnosis and gene discovery. Challenge predictors were provided with a dataset of variant calls and phenotype terms from 175 RGP individuals (65 families), including 35 solved training set families with causal variants specified, and 30 unlabeled test set families (14 solved, 16 unsolved). We tasked teams to identify causal variants in as many families as possible. Predictors submitted variant predictions with estimated probability of causal relationship (EPCR) values. Model performance was determined by two metrics, a weighted score based on the rank position of causal variants, and the maximum F-measure, based on precision and recall of causal variants across all EPCR values.
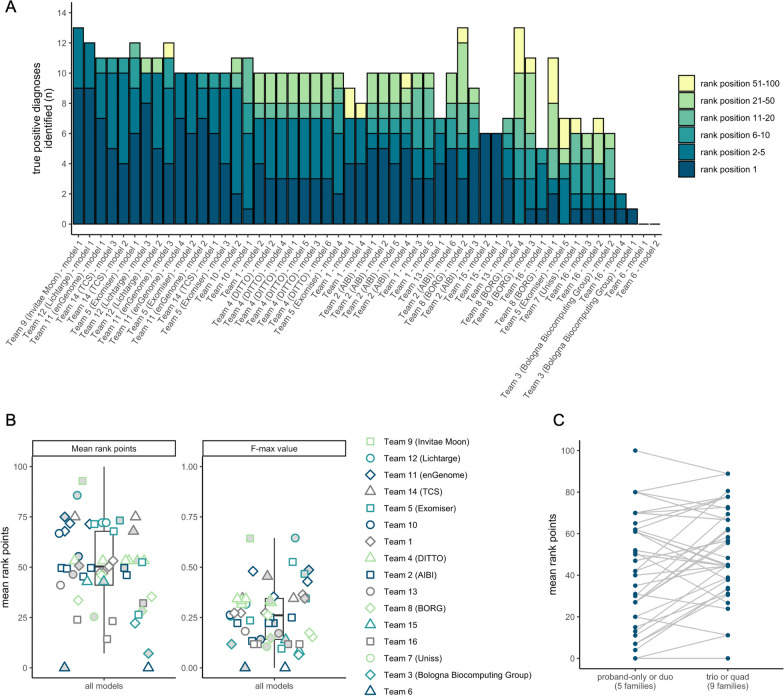
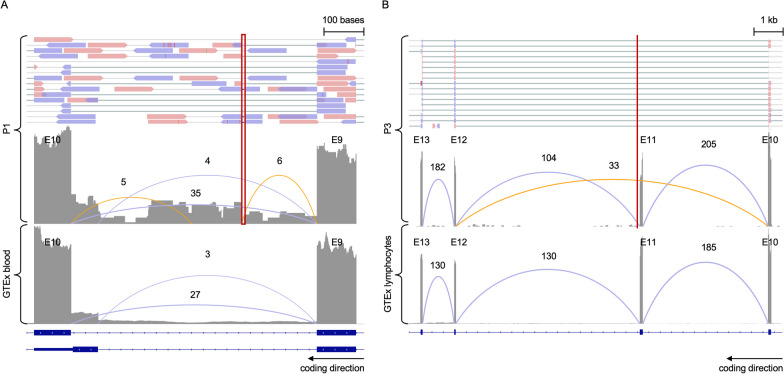
Results: Sixteen teams submitted predictions from 52 models, some with manual review incorporated. Top performers recalled causal variants in up to 13 of 14 solved families within the top 5 ranked variants. Newly discovered diagnostic variants were returned to two previously unsolved families following confirmatory RNA sequencing, and two novel disease gene candidates were entered into Matchmaker Exchange. In one example, RNA sequencing demonstrated aberrant splicing due to a deep intronic indel in ASNS, identified in trans with a frameshift variant in an unsolved proband with phenotypes consistent with asparagine synthetase deficiency.
Conclusions: Model methodology and performance was highly variable. Models weighing call quality, allele frequency, predicted deleteriousness, segregation, and phenotype were effective in identifying causal variants, and models open to phenotype expansion and non-coding variants were able to capture more difficult diagnoses and discover new diagnoses. Overall, computational models can significantly aid variant prioritization. For use in diagnostics, detailed review and conservative assessment of prioritized variants against established criteria is needed.
Keywords: Best practices; Genome interpretation; Genome sequencing; Rare disease; Variant prioritization.
© 2024. The Author(s).
Conflict of interest statement
Authors S.Z., I.L., E.R., P.M., and R.B., own shares of enGenome srl. Authors F.D.P. and G.N. are employees of enGenome srl. Authors T.J., R.S., S.G.V., N.S., A.R., U.S., N.T., are employees of TCS Ltd. Authors P.J.C., C.K., K.N., and P.S. are employees of Invitae Ltd. H.L.R. receives support from Illumina and Microsoft for rare disease gene discovery and diagnosis. A.O’D-L. is a member of the scientific advisory board for Congenica Inc and chairs the clinical advisory board for CAGI. S.E.B receives support at UC Berkeley from a research agreement from TCS. All other authors report no competing interests.
Figures
Update of
-
Critical assessment of variant prioritization methods for rare disease diagnosis within the Rare Genomes Project.medRxiv [Preprint]. 2023 Aug 4:2023.08.02.23293212. doi: 10.1101/2023.08.02.23293212. medRxiv. 2023. Update in: Hum Genomics. 2024 Apr 29;18(1):44. doi: 10.1186/s40246-024-00604-w. PMID: 37577678 Free PMC article. Updated. Preprint.
References
-
- Clark MM, Stark Z, Farnaes L, Tan TY, White SM, Dimmock D, et al. Meta-analysis of the diagnostic and clinical utility of genome and exome sequencing and chromosomal microarray in children with suspected genetic diseases. NPJ Genom Med. 2018;9(3):16. doi: 10.1038/s41525-018-0053-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
