

TROPION-Breast03: a randomized phase III global trial of datopotamab deruxtecan ± durvalumab in patients with triple-negative breast cancer and residual invasive disease at surgical resection after neoadjuvant therapy
- PMID: 38686016
- PMCID: PMC11057345
- DOI: 10.1177/17588359241248336
TROPION-Breast03: a randomized phase III global trial of datopotamab deruxtecan ± durvalumab in patients with triple-negative breast cancer and residual invasive disease at surgical resection after neoadjuvant therapy
Abstract
Background: Despite advances in the treatment of early triple-negative breast cancer (TNBC), patients with residual invasive disease after neoadjuvant therapy have a high risk of disease recurrence and worse survival outcomes than those who have pathological complete response (pCR). Improving outcomes in early TNBC remains an unmet need requiring new adjuvant treatment approaches. Datopotamab deruxtecan (Dato-DXd) is an antibody-drug conjugate comprising a humanized anti-trophoblast cell-surface antigen 2 immunoglobulin G1 (IgG1) monoclonal antibody attached via a plasma-stable, cleavable linker to a potent topoisomerase I inhibitor payload, with activity observed in advanced TNBC.
Objectives: TROPION-Breast03 is an ongoing phase III study evaluating the efficacy and safety of Dato-DXd alone or combined with durvalumab versus standard-of-care therapy as adjuvant treatment in patients with stage I-III TNBC with residual invasive disease at surgical resection following neoadjuvant treatment.
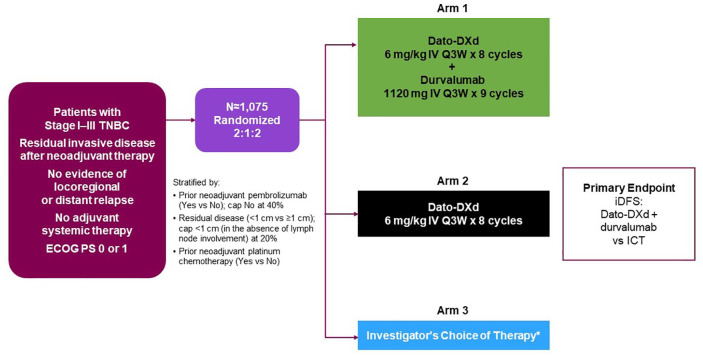
Methods and design: Eligible patients, aged ⩾18 years, will be randomized in a 2:1:2 ratio to receive Dato-DXd [6 mg/kg intravenously (IV) every 3 weeks (Q3W); eight cycles] and durvalumab (1120 mg IV Q3W; nine cycles), Dato-DXd monotherapy (6 mg/kg IV Q3W), or investigator's choice of therapy (ICT; capecitabine, pembrolizumab, or capecitabine and pembrolizumab). The primary endpoint is invasive disease-free survival (iDFS) for Dato-DXd and durvalumab versus ICT. Key secondary endpoints include safety, distant disease-free survival, and overall survival for Dato-DXd and durvalumab versus ICT and iDFS for Dato-DXd monotherapy versus ICT.
Ethics: TROPION-Breast03 will be approved by the independent ethics committees or institutional review boards at each study site. All study participants will provide written informed consent.
Discussion: TROPION-Breast03 will help define the potential role of Dato-DXd in the treatment of patients with early-stage TNBC who do not have pCR after neoadjuvant therapy.
Trial registration: ClinicalTrials.gov identifier: NCT05629585 (registration date: 29 November 2022).
Keywords: adjuvant therapy; antibody–drug conjugates; immunotherapy; programmed cell death ligand-1; triple-negative breast cancer; trophoblast cell-surface antigen 2.
Plain language summary
TROPION-Breast03: a clinical trial designed to assess the effectiveness and safety of Dato-DXd, alone or in combination with durvalumab, in patients with triple-negative breast cancer who have cancer cells remaining at the time of surgery after initial systemic therapy Triple-negative breast cancer (TNBC), in which cells do not have estrogen or progesterone receptors or high levels of human epidermal growth factor receptor 2, is the most aggressive breast cancer subtype. TNBC is difficult to treat and associated with high risk of recurrence despite standard systemic therapy (treatment targeting the entire body), which can include chemotherapy alone or in combination with immunotherapy (treatment targeting the immune system). To reduce the risk of recurrence, standard systemic treatment is often followed by surgical removal of the patient’s tumors and additional systemic treatment. Dato-DXd is an antibody-drug conjugate, which is an anticancer drug (DXd) connected to an antibody (datopotamab) by a stable linker. Datopotamab binds to TROP2, a protein found on breast cancer cells, and is taken into the tumor cell where the linker breaks, releasing DXd to kill the cell. By delivering DXd directly to cancer cells, Dato-DXd reduces exposure in the rest of the body, reducing the risk of side effects. Since Dato-DXd can recruit immune cells to cancer sites, it may work better combined with durvalumab, a drug that blocks the activity of a protein called PD-L1, making cancer cells more susceptible to being killed by immune cells. The TROPION-Breast03 study will compare Dato-DXd, alone or combined with durvalumab, with standard-of-care therapy in patients with TNBC that has not spread to parts of the body away from the original tumor site(s), but with cancer cells remaining at the time of surgery after initial systemic therapy. It will assess how well each treatment works and describe any side effects. We plan to recruit 1,075 eligible adults who will be randomly assigned in a 2:1:2 ratio to: • Dato-DXd + durvalumab • Dato-DXd alone • Standard-of-care therapy • Patients will receive treatment until they complete the planned course of therapy (8 or 9 cycles), their cancer returns, side effects become unacceptable, or they choose to stop.
© The Author(s), 2024.
Conflict of interest statement
A.B. reports consulting fees from Pfizer, Novartis, Genentech, Merck, Radius Health, Immunomedics/Gilead, Sanofi, Daiichi Pharma/AstraZeneca, Phillips, Eli Lilly, and Foundation Medicine; grants or funds from Genentech, Novartis, Pfizer, Merck, Sanofi, Radius Health, Immunomedics/Gilead, Daiichi Pharma/AstraZeneca, and Eli Lilly. L.P. reports membership on the board of directors for the HOPE Foundation; consulting fees from Pfizer, AstraZeneca, Merck, Novartis, Bristol Myers Squibb, GlaxoSmithKline, Roche/Genentech, Personalis, Daiichi, Natera, and Exact Sciences; and institutional research funding from Seagen, GlaxoSmithKline, AstraZeneca, Merck, Pfizer, and Bristol Myers Squibb. K.A. reports institutional research funding from Quantum Leap (I-SPY 2); and non-financial conflicts with IDMC (member) and Seattle Genetics. EMC reports consulting fees from Pfizer, MSD, Gilead, Roche, Eli Lilly, Daiichi-Sankyo, Novartis, and AstraZeneca; and institutional research funding from Roche. S.-A.I. reports advisory council or committee participation with AstraZeneca, Novartis, Hanmi, Pfizer, Eisai, Roche, Eli Lilly, GlaxoSmithKline, MSD, Daiichi-Sankyo, Idience, and Bertis; and grants or funds from AstraZeneca, Pfizer, Eisai, Roche, Daewoong Pharm, Boryung Pharm, and Daiichi-Sankyo. D.H. declares no conflicts of interest. K.K. reports consulting fees from Merck, Eli Lilly, Novartis, AstraZeneca, Roche/Genentech, Immunomedics, Seattle Genetics, Oncosec, 4D pharma, Daiichi-Sankyo, Puma Biotechnology, Mersna, Menarini Silicon Biosystems, Myovant Sciences, and Takeda; and grants or funds from Novartis, Ascentage, Roche/Genentech, Eli Lilly, Seattle Genetics, AstraZeneca, and Daiichi-Sankyo. C.I. reports consulting fees from Genentech, Puma Biotechnology, Seattle Genetics, AstraZeneca, Novartis, Pfizer, ION, and Gilead; institutional research funding from Tesaro/GlaxoSmithKline, Seattle Genetics, Pfizer, AstraZeneca, Bristol Myers Squibb, Genentech, and Novartis; and other financial relationships with Wolters Kluwer (UptoDate) and McGraw Hill (Goodman and Gillman). D.L. reports advisory council or committee participation with MSD, Seagen, Novartis, Eli Lilly, AstraZeneca, and Exact Sciences; honoraria from MSD, Seagen, Pfizer, Novartis, Eli Lilly, AstraZeneca, Roche, Exact Sciences, and Daiichi-Sankyo; and consulting fees from MSD and AstraZeneca. L.T. reports advisory council or committee participation with AstraZeneca, Daichii-Sankyo, MSD, Eli Lilly, Novartis, and Pfizer; consulting fees from AstraZeneca, Daiichi-Sankyo, MSD, Novartis, and Pfizer; grants or funds from Novartis; and provision of educational support for Roche, Pfizer, AstraZeneca, and Gilead. E.T. reports honoraria from Daiichi-Sankyo, AstraZeneca, and Eli Lilly. J.W. reports research funding from the National Natural Science Foundation and F. Hoffmann-La Roche Ltd; committee participation with Eli Lilly, AstraZeneca; honoraria from Novartis. H.D. reports employment by AstraZeneca and ownership of stock/shares in AstraZeneca. W.B. declares no conflicts of interest. R.K. reports employment by AstraZeneca. M.M. reports employment by AstraZeneca and ownership of stock/shares in AstraZeneca. N.H. reports membership on the board of directors of the West German Study Group (WSG); status as the ESMO Director of Education; honoraria from Amgen, AstraZeneca, Daiichi-Sankyo, EPG Communication, Gilead, Eli Lilly, Medscape, MSD, Novartis, Pierre-Fabre, Pfizer, Roche, Sandoz, Sanofi, Seagen, Springer, Viatris, and Zuellig Pharma; consulting fees from Gilead, Roche, Sandoz, Sanofi, and Seagen. P.S. reports consulting fees from Pfizer, Merck, Gilead, Genzyme (Sanofi), Novartis, AstraZeneca, and GlaxoSmithKline; institutional research funding from Novartis, Merck, and Gilead; and royalties from UpToDate.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of Incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209–249. - PubMed
-
- Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res 2007; 13: 4429–4434. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
