

Endobronchial Ultrasound Guided Transbronchial Needle Aspiration and Next Generation Sequencing Yields
- PMID: 38687384
- PMCID: PMC11143046
- DOI: 10.1007/s00408-024-00690-6
Endobronchial Ultrasound Guided Transbronchial Needle Aspiration and Next Generation Sequencing Yields
Abstract
Purpose: The use of endobronchial ultrasound (EBUS) is standard practice for lung cancer diagnosis and staging. Next generation sequencing (NGS) for detection of genetic alterations is recommended in advanced, non-squamous, non-small-cell lung cancer (NSCLC). Existing protocols for NGS testing are minimal and reported yields vary. This study aimed to determine the yield of EBUS samples obtained for NGS using a sampling protocol at our institution and assess predictive factors to form collection protocols.
Methods: We reviewed EBUS bronchoscopies from 2016 to 2021 with non-squamous NSCLC diagnoses. For target lesions suspected to be malignant, the sampling protocol was: (a) two slides for on-site evaluation, (b) three to five fine needle aspirations rinsed into saline for immunohistochemical staining and in-house molecular markers, and (c) additional three to five rinses for NGS. Sufficiency for NGS processing was determined by the pathology department.
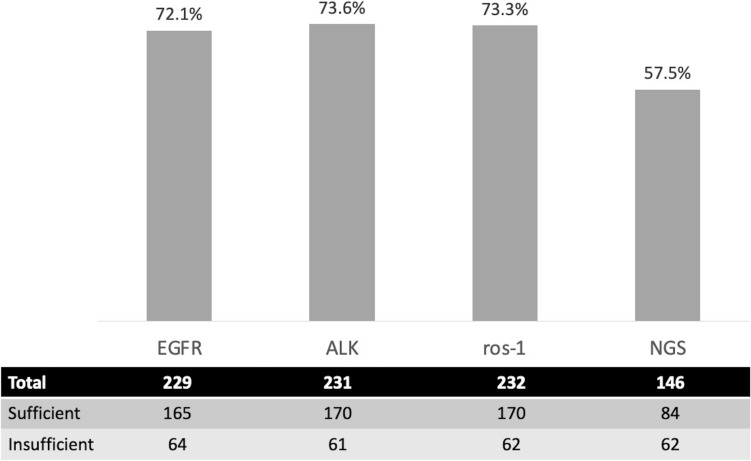
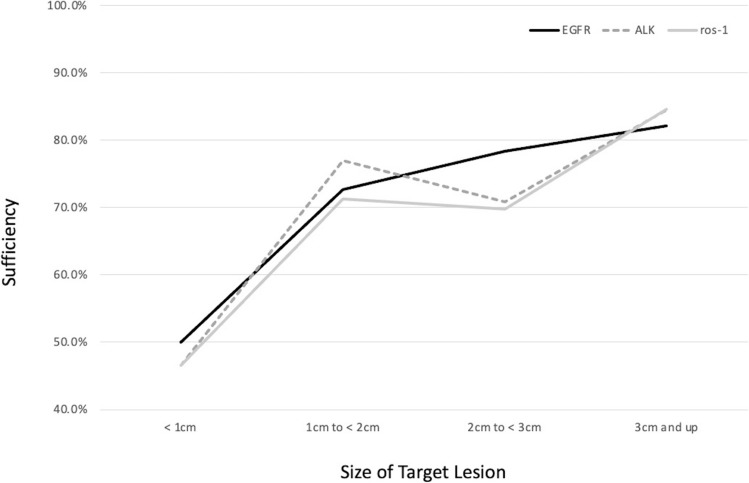
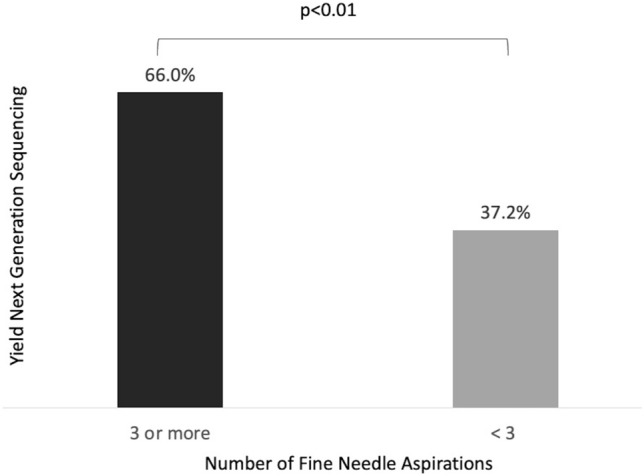
Results: Two hundred and seventy-eight non-squamous NSCLC samples were obtained by EBUS (205 adenocarcinoma; 73 not otherwise specified). EBUS was performed under general anesthesia in 75.5% of cases. The overall sample adequacy for NGS testing was 57.5%. Higher adequacy rates were observed when protocol was adhered to 66.0% versus 37.2% (p < 0.001). There was no statistically significant difference based on the size of the lesion or location of the sample.
Conclusion: When a protocol of three to five dedicated needle rinses for NGS was followed, we nearly doubled our sample adequacy rate for NSG as compared to standard care. Studies are needed to determine the ideal collection and processing modality to preserve tissue samples for genetic sequencing.
Keywords: Bronchoscopy; EBUS-TBNA; Lung cancer; Molecular markers; Next generation sequencing.
© 2024. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures


Similar articles
-
Endobronchial Ultrasound Guided Transbronchial Needle Aspiration and PD-L1 Yields.Lung. 2024 Jun;202(3):325-330. doi: 10.1007/s00408-024-00692-4. Epub 2024 Apr 18. Lung. 2024. PMID: 38637361 Free PMC article.
-
Usefulness of endoscopic ultrasound with bronchoscope-guided fine-needle aspiration for next-generation sequencing in patients with non-small cell lung cancer: A comparison with other bronchoscopic techniques.Respir Investig. 2024 Sep;62(5):879-883. doi: 10.1016/j.resinv.2024.07.012. Epub 2024 Aug 2. Respir Investig. 2024. PMID: 39096541
-
The Performance of an Extended Next Generation Sequencing Panel Using Endobronchial Ultrasound-Guided Fine Needle Aspiration Samples in Non-Squamous Non-Small Cell Lung Cancer: A Pragmatic Study.Clin Lung Cancer. 2023 Mar;24(2):e105-e112. doi: 10.1016/j.cllc.2022.11.010. Epub 2022 Dec 5. Clin Lung Cancer. 2023. PMID: 36599742 Free PMC article. Clinical Trial.
-
A systematic review and meta-analysis of the adequacy of endobronchial ultrasound transbronchial needle aspiration for next-generation sequencing in patients with non-small cell lung cancer.Lung Cancer. 2022 Apr;166:17-26. doi: 10.1016/j.lungcan.2022.01.018. Epub 2022 Jan 25. Lung Cancer. 2022. PMID: 35151114
-
Comparing diagnostic sensitivity of different needle sizes for lymph nodes suspected of lung cancer in endobronchial ultrasound transbronchial needle aspiration: Systematic review and meta-analysis.Clin Respir J. 2021 Dec;15(12):1328-1336. doi: 10.1111/crj.13436. Epub 2021 Aug 31. Clin Respir J. 2021. PMID: 34402194
Cited by
-
Liquid biopsy in lung cancer.Breathe (Sheff). 2025 Aug 19;21(3):250051. doi: 10.1183/20734735.0051-2025. eCollection 2025 Jul. Breathe (Sheff). 2025. PMID: 40837417 Free PMC article. Review.
-
Factors influencing the diagnostic accuracy of lung cancer using endobronchial ultrasound-guided transbronchial needle aspiration.Am J Transl Res. 2025 Apr 15;17(4):2690-2700. doi: 10.62347/UIGU6267. eCollection 2025. Am J Transl Res. 2025. PMID: 40385055 Free PMC article.
-
LUNG Year in Review: 2024.Lung. 2025 Jan 22;203(1):29. doi: 10.1007/s00408-025-00785-8. Lung. 2025. PMID: 39841240 No abstract available.
References
-
- Navani N, Nankivell M, Lawrence DR, et al. Lung cancer diagnosis and staging with endobronchial ultrasound-guided transbronchial needle aspiration compared with conventional approaches: an open-label, pragmatic, randomized controlled trial. Lancet. 2015;3(4):282–289. doi: 10.1016/S2213-2600(15)00029-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
