

Rational treatment options for T1/2N0M0 squamous cell carcinoma of the anal canal: a population-based study combined with external validation
- PMID: 38688457
- PMCID: PMC11299955
- DOI: 10.1093/oncolo/oyae068
Rational treatment options for T1/2N0M0 squamous cell carcinoma of the anal canal: a population-based study combined with external validation
Abstract
Background: Treatment options for T1/2N0M0 anal squamous cell carcinoma include chemotherapy, radiotherapy, chemoradiotherapy, and local excision, although the optimal treatment method has not been determined.
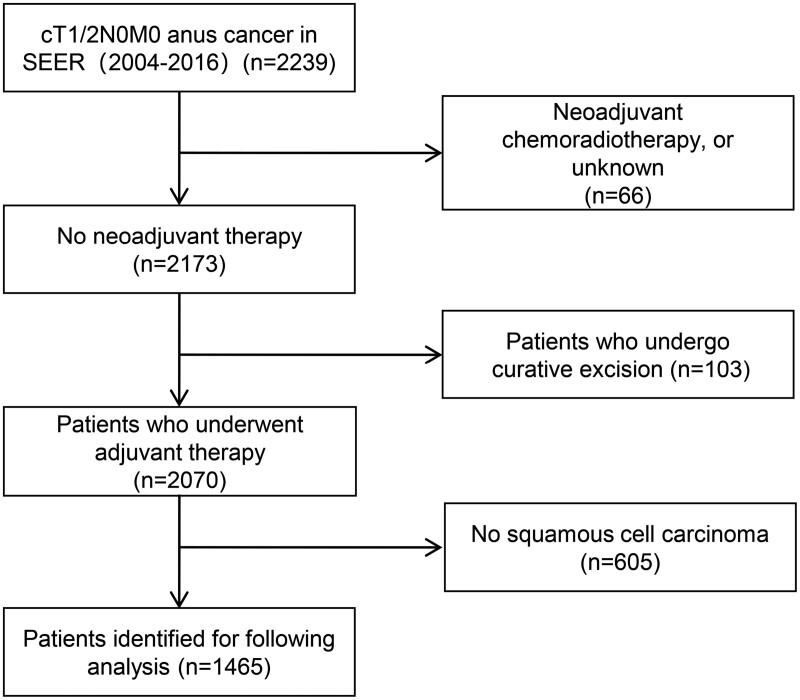
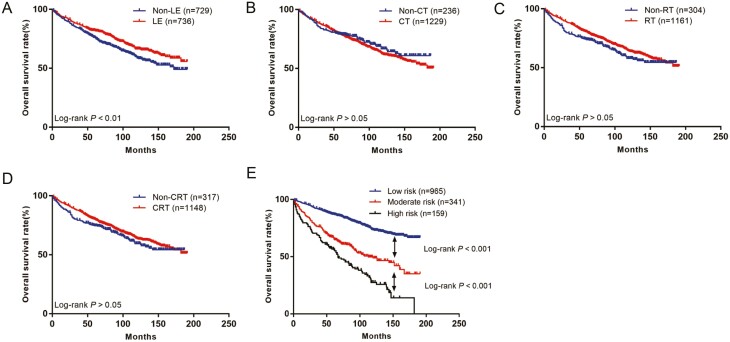
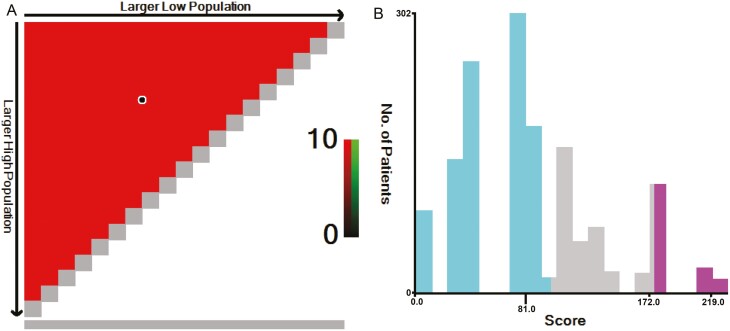
Methods: The National Cancer Institute Surveillance, Epidemiology and Results database was used to search and screen 1465 patients with cT1/2N0M0 anal squamous cell carcinoma who were clinically diagnosed between 2004 and 2016. Survival analysis was performed using the Kaplan-Meier method and log-rank test. Cox proportional hazards regression analysis was performed to screen independent prognostic factors and build a nomogram survival prediction model. According to the risk score, patients were divided into low, medium, and high risk groups using X-tile software.
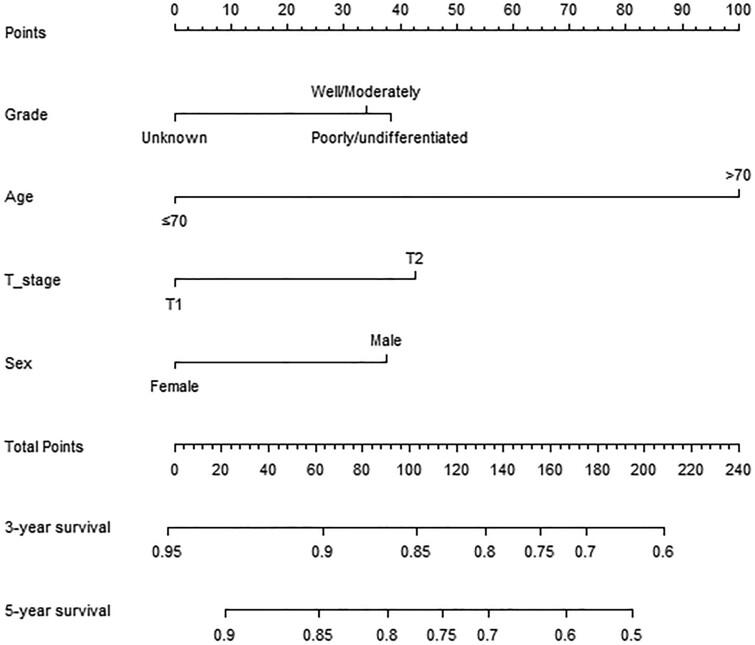
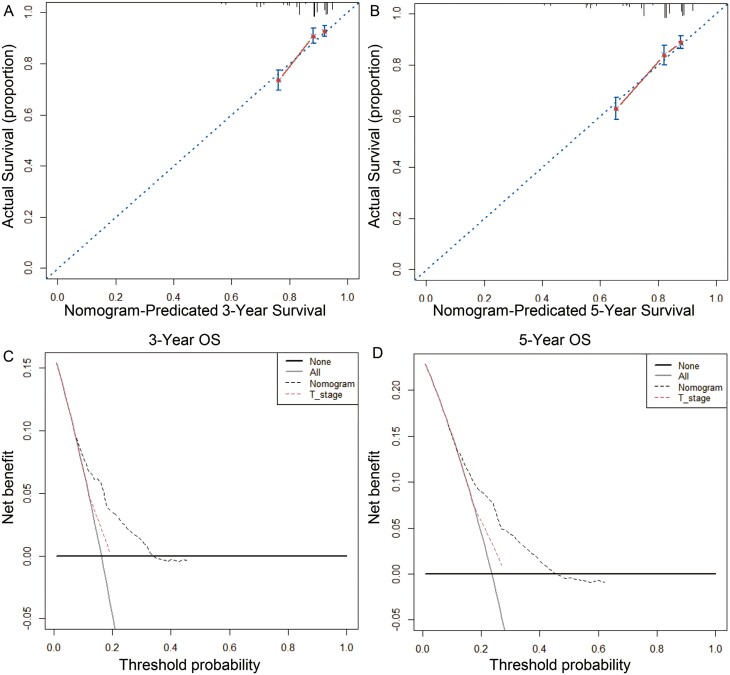
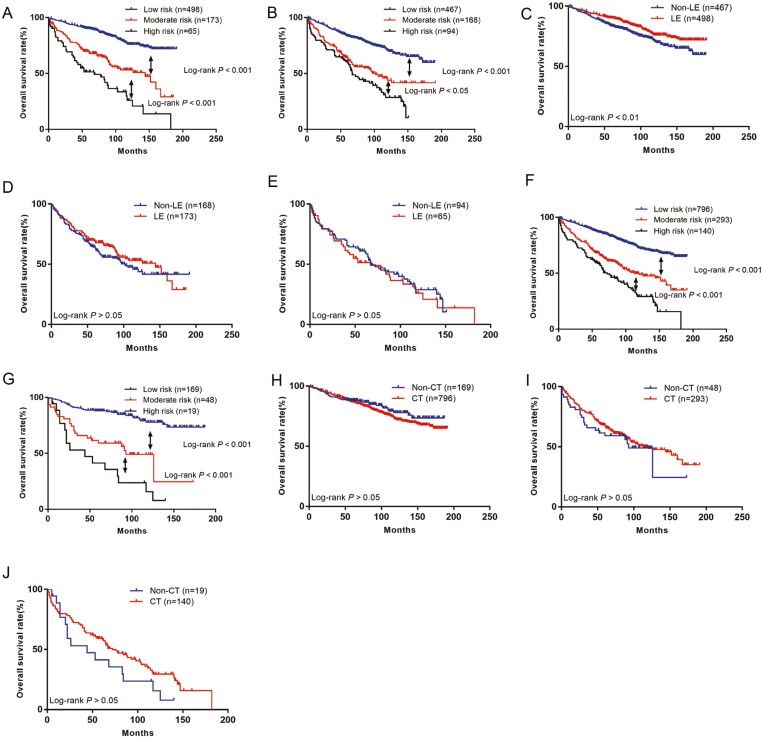
Results: Age, sex, grade and cT stage were identified as independent prognostic factors for cT1/2N0M0 anal squamous cell carcinoma and were included in the nomogram to construct a prediction model. The C-index of the model was 0.770 [95% confidence interval (CI), 0.693-0.856], which was higher than the C-index of T stage 0.565 (95% CI, 0.550-0.612). Low-risk patients benefited from local resection, moderate-risk patients benefited from radiotherapy, and high-risk patients benefited from radiotherapy or chemoradiotherapy. This was confirmed using external validation data from the center.
Conclusion: The nomogram developed in this study effectively and comprehensively evaluated the prognosis of patients with cT1/2N0M0 squamous cell carcinoma of the anal canal. Local excision is recommended for low risk patients, radiotherapy for moderate-risk patients, and radiotherapy or chemoradiotherapy for high-risk patients.
Keywords: cT1/2N0M0 squamous cell carcinoma of the anal canal; nomogram; prognosis; rational treatment.
© The Author(s) 2024. Published by Oxford University Press.
Conflict of interest statement
The authors indicated no financial relationships.
Figures
Similar articles
-
Construction and validation of a prognostic nomogram for anal squamous cell carcinoma.Cancer Med. 2022 Jan;11(2):392-405. doi: 10.1002/cam4.4458. Epub 2021 Dec 1. Cancer Med. 2022. PMID: 34850581 Free PMC article.
-
Comparative Survival of Patients With Anal Adenocarcinoma, Squamous Cell Carcinoma of the Anus, and Rectal Adenocarcinoma.Clin Colorectal Cancer. 2016 Mar;15(1):47-53. doi: 10.1016/j.clcc.2015.07.007. Epub 2015 Aug 1. Clin Colorectal Cancer. 2016. PMID: 26362848
-
Comparison of the TNM9th and 8th editions for localized and locally advanced anal squamous cell carcinoma treated nonsurgically and proposal of a new stage grouping system.Cancer Med. 2024 Aug;13(16):e70119. doi: 10.1002/cam4.70119. Cancer Med. 2024. PMID: 39158000 Free PMC article.
-
Malignant tumors of the anal canal: the spectrum of disease, treatment, and outcomes.Cancer. 1999 Apr 15;85(8):1686-93. doi: 10.1002/(sici)1097-0142(19990415)85:8<1686::aid-cncr7>3.0.co;2-7. Cancer. 1999. PMID: 10223561 Review.
-
Chemoradiotherapy for anal squamous cell carcinoma.Surgeon. 2016 Aug;14(4):202-12. doi: 10.1016/j.surge.2016.03.006. Epub 2016 Apr 23. Surgeon. 2016. PMID: 27118047 Review.
Cited by
-
Prognosis Prediction and Surgical Benefit Subgroup Analysis in Anal Squamous Cell Carcinoma Patients Undergoing Concurrent Chemoradiotherapy.Cancer Med. 2025 Aug;14(15):e71091. doi: 10.1002/cam4.71091. Cancer Med. 2025. PMID: 40787842 Free PMC article.
References
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
