

Prediagnostic plasma proteomics profile for hepatocellular carcinoma
- PMID: 38688524
- PMCID: PMC11308170
- DOI: 10.1093/jnci/djae079
Prediagnostic plasma proteomics profile for hepatocellular carcinoma
Abstract
Objective: Proteomics may discover pathophysiological changes related to hepatocellular carcinoma, an aggressive and lethal type of cancer with low sensitivity for early stage diagnosis.
Design: We measured 1305 prediagnostic (median = 12.7 years) SomaScan proteins from 54 pairs of healthy individuals who subsequently developed hepatocellular carcinoma and matched non-hepatocellular carcinoma control individuals from the Nurses' Health Study (NHS) and the Health Professionals Follow-up Study (HPFS). Candidate proteins were validated in the independent, prospective UK Biobank Pharma Proteomics Project (UKB-PPP).
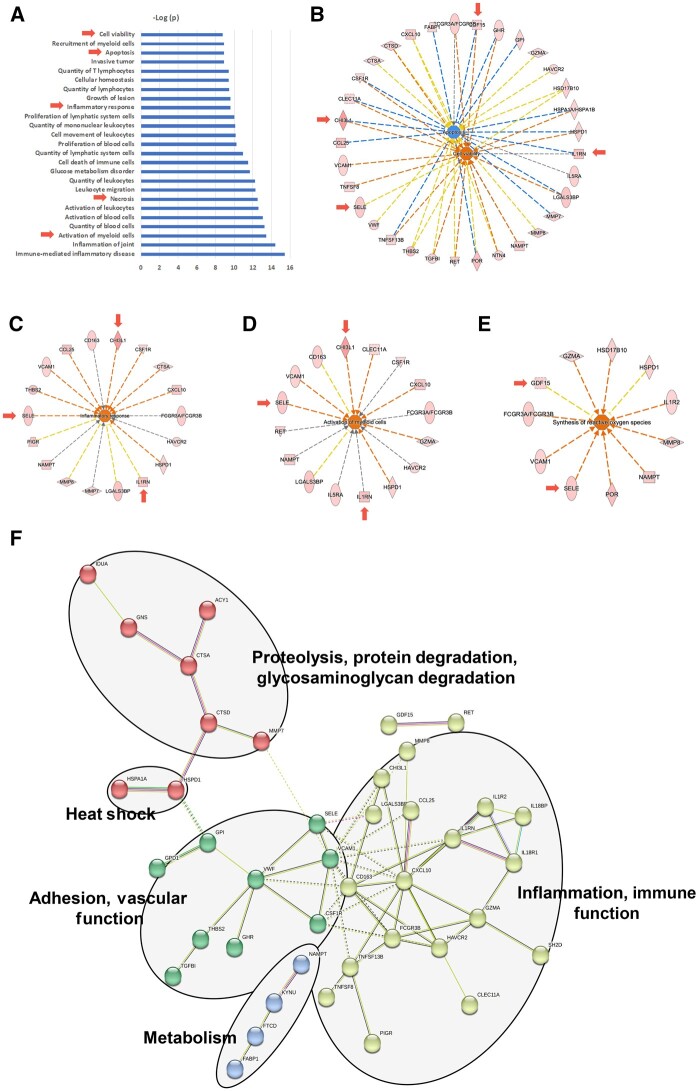
Results: In NHS and HPFS, we identified 56 elevated proteins in hepatocellular carcinoma with an absolute fold change of more than 1.2 and a Wald test P value less than .05 in conditional logistic regression analysis. Ingenuity pathway analysis identified enrichment of pathways associated with cell viability, adhesion, proteolysis, apoptosis, and inflammatory response. Four proteins-chitinase-3-like protein 1, growth differentiation factor 15, interleukin-1 receptor antagonist protein, and E-selectin-showed strong positive associations with hepatocellular carcinoma and were thus validated by enzyme-linked immunosorbent assay (odds ratio = 2.48-14.7, all P < .05) in the NHS and HPFS and by Olink platform (hazard ratio = 1.90-3.93, all P < .05) in the UKB-PPP. Adding these 4 proteins to a logistic regression model of traditional hepatocellular carcinoma risk factors increased the area under the curve from 0.67 to 0.87 in the NHS and HPFS. Consistently, model area under the curve was 0.88 for hepatocellular carcinoma risk prediction in the UKB-PPP.
Conclusion: However, the limited number of hepatocellular carcinoma patients in the cohorts necessitates caution in interpreting our findings, emphasizing the need for further validation in high-risk populations.
© The Author(s) 2024. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
Dr Andrew T. Chan served as a consultant for Bayer Pharma AG, Pfizer Inc, and Boehringer Ingelheim for work unrelated to this topic. He has also received grant support from Pfizer Inc, Zoe Ltd, and Freenome for work unrelated to this topic.
Figures



References
-
- National Cancer Institute. SEER Cancer Stat Facts: Liver and Intrahepatic Bile Duct Cancer, 1992-2022. https://seer.cancer.gov/statfacts/html/livibd.html. Accessed February 8, 2023.
MeSH terms
Substances
Grants and funding
- Harvard Cancer Center Cancer Proteomics Core
- R37 CA262299/CA/NCI NIH HHS/United States
- U01 CA272452/CA/NCI NIH HHS/United States
- P01 CA087969/CA/NCI NIH HHS/United States
- P30 CA006516/GF/NIH HHS/United States
- HPFS
- BIDMC Genomics, Proteomics, Bioinformatics and Systems Biology Center
- American Cancer Society Clinical Research Professor
- R21 CA238651/CA/NCI NIH HHS/United States
- PASD-22-1003396-01-PASD/ACS Interdisciplinary Team
- NH/NIH HHS/United States
- RSG-17-190-01-NEC/Research Scholar Award
- R21 CA252962/CA/NCI NIH HHS/United States
- UM1 CA186107/CA/NCI NIH HHS/United States
- R01 CA049449/CA/NCI NIH HHS/United States
- R35 CA253185/CA/NCI NIH HHS/United States
- The Dana Farber
- U01 CA259208/CA/NCI NIH HHS/United States
- P30 CA006516/CA/NCI NIH HHS/United States
- American Cancer Society
LinkOut - more resources
Full Text Sources
Medical
Research Materials
