

TLR7-dependent eosinophil degranulation links psoriatic skin inflammation to small intestinal inflammatory changes in mice
- PMID: 38689088
- PMCID: PMC11148187
- DOI: 10.1038/s12276-024-01225-y
TLR7-dependent eosinophil degranulation links psoriatic skin inflammation to small intestinal inflammatory changes in mice
Abstract
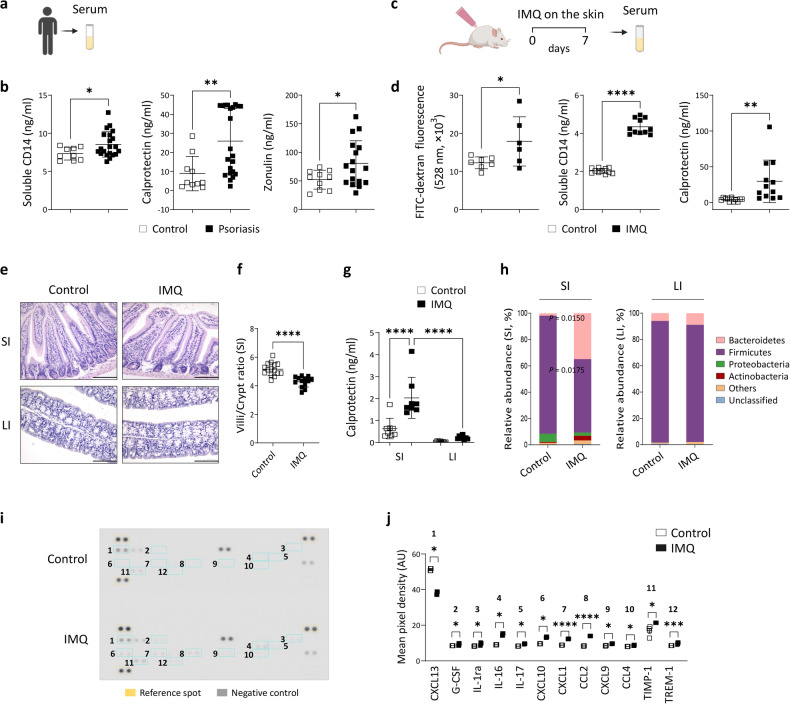
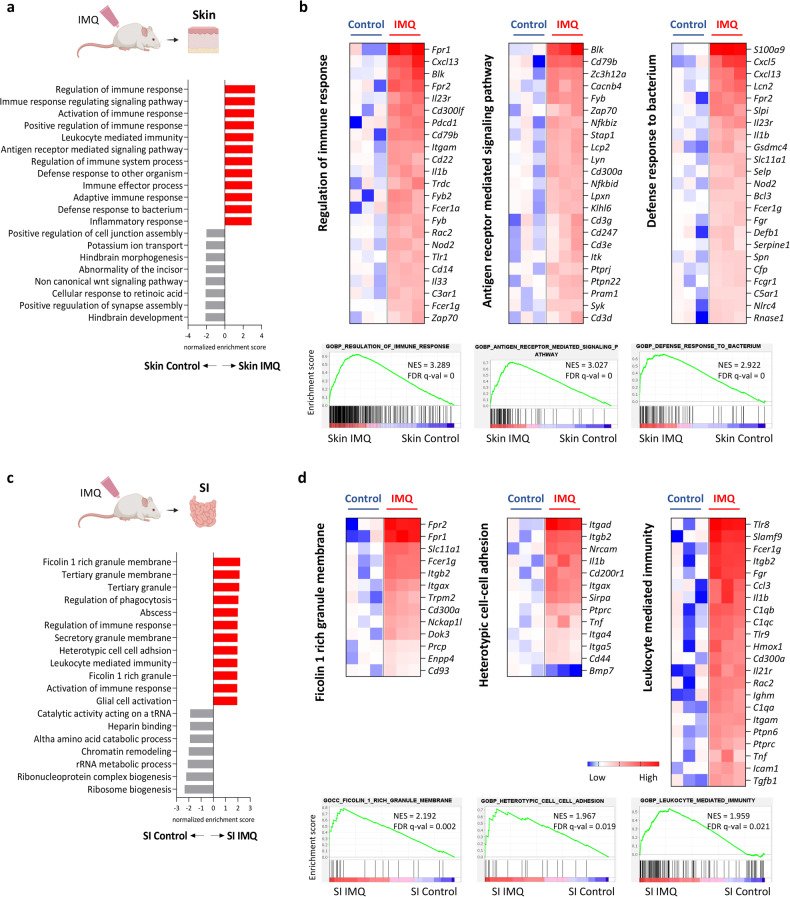
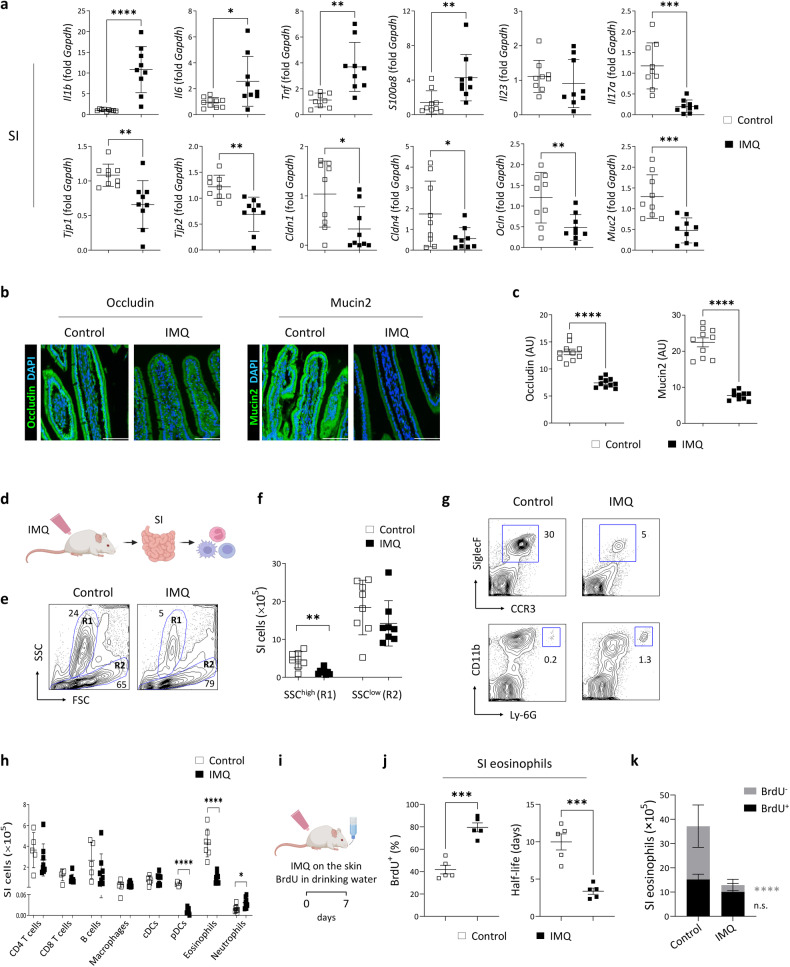
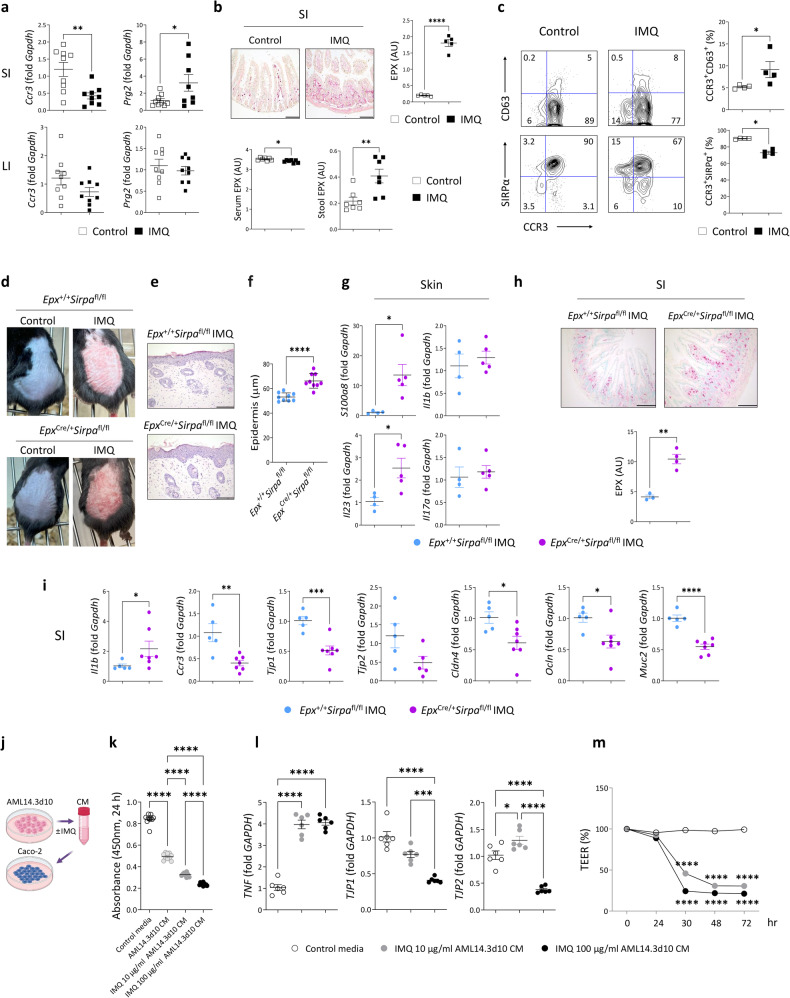
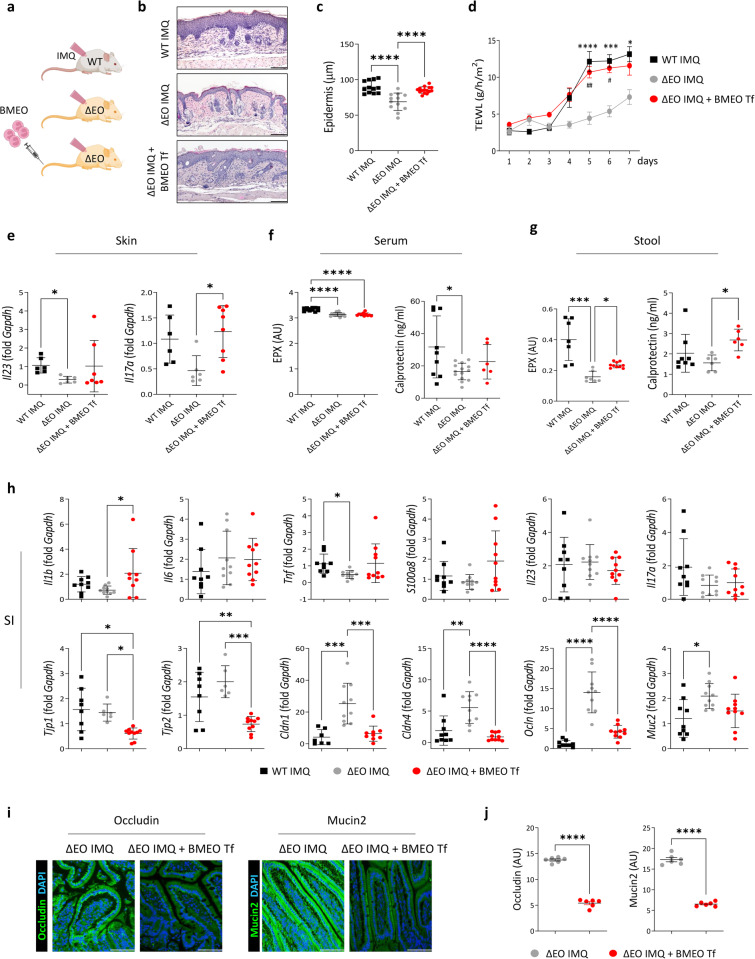
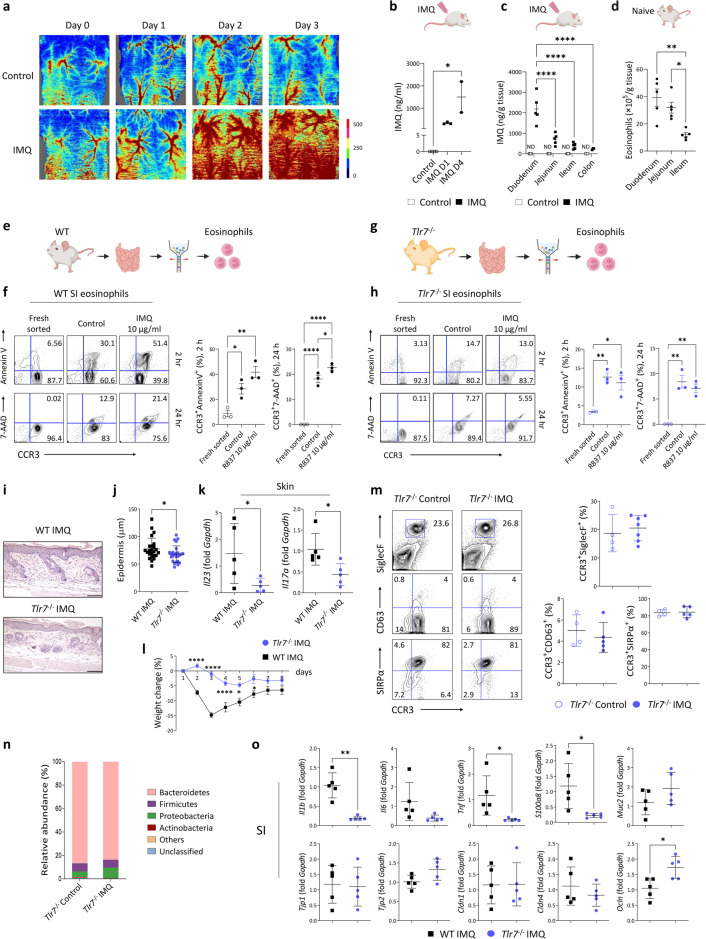
Recent evidence of gut microbiota dysbiosis in the context of psoriasis and the increased cooccurrence of inflammatory bowel disease and psoriasis suggest a close relationship between skin and gut immune responses. Using a mouse model of psoriasis induced by the Toll-like receptor (TLR) 7 ligand imiquimod, we found that psoriatic dermatitis was accompanied by inflammatory changes in the small intestine associated with eosinophil degranulation, which impaired intestinal barrier integrity. Inflammatory responses in the skin and small intestine were increased in mice prone to eosinophil degranulation. Caco-2 human intestinal epithelial cells were treated with media containing eosinophil granule proteins and exhibited signs of inflammation and damage. Imiquimod-induced skin and intestinal changes were attenuated in eosinophil-deficient mice, and this attenuation was counteracted by the transfer of eosinophils. Imiquimod levels and the distribution of eosinophils were positively correlated in the intestine. TLR7-deficient mice did not exhibit intestinal eosinophil degranulation but did exhibit attenuated inflammation in the skin and small intestine following imiquimod administration. These results suggest that TLR7-dependent bidirectional skin-to-gut communication occurs in psoriatic inflammation and that inflammatory changes in the intestine can accelerate psoriasis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
