

Intermittent intravenous paracetamol versus continuous morphine in infants undergoing cardiothoracic surgery: a multi-center randomized controlled trial
- PMID: 38689310
- PMCID: PMC11061924
- DOI: 10.1186/s13054-024-04905-3
Intermittent intravenous paracetamol versus continuous morphine in infants undergoing cardiothoracic surgery: a multi-center randomized controlled trial
Abstract
Background: To determine whether intermittent intravenous (IV) paracetamol as primary analgesic would significantly reduce morphine consumption in children aged 0-3 years after cardiac surgery with cardiopulmonary bypass.
Methods: Multi-center, randomized, double-blinded, controlled trial in four level-3 Pediatric Intensive Care Units (PICU) in the Netherlands and Belgium. Inclusion period; March 2016-July 2020. Children aged 0-3 years, undergoing cardiac surgery with cardiopulmonary bypass were eligible. Patients were randomized to continuous morphine or intermittent IV paracetamol as primary analgesic after a loading dose of 100 mcg/kg morphine was administered at the end of surgery. Rescue morphine was given if numeric rating scale (NRS) pain scores exceeded predetermined cutoff values. Primary outcome was median weight-adjusted cumulative morphine dose in mcg/kg in the first 48 h postoperative. For the comparison of the primary outcome between groups, the nonparametric Van Elteren test with stratification by center was used. For comparison of the proportion of patients with one or more NRS pain scores of 4 and higher between the two groups, a non-inferiority analysis was performed using a non-inferiority margin of 20%.
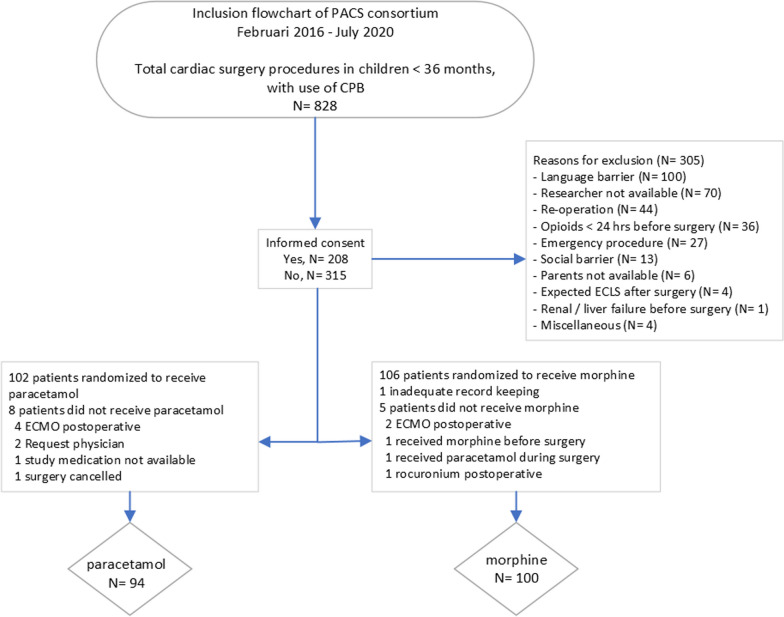
Results: In total, 828 were screened and finally 208 patients were included; parents of 315 patients did not give consent and 305 were excluded for various reasons. Fourteen of the enrolled 208 children were withdrawn from the study before start of study medication leaving 194 patients for final analysis. One hundred and two patients received intermittent IV paracetamol, 106 received continuous morphine. The median weight-adjusted cumulative morphine consumption in the first 48 h postoperative in the IV paracetamol group was 5 times lower (79%) than that in the morphine group (median, 145.0 (IQR, 115.0-432.5) mcg/kg vs 692.6 (IQR, 532.7-856.1) mcg/kg; P < 0.001). The rescue morphine consumption was similar between the groups (p = 0.38). Non-inferiority of IV paracetamol administration in terms of NRS pain scores was proven; difference in proportion - 3.1% (95% CI - 16.6-10.3%).
Conclusions: In children aged 0-3 years undergoing cardiac surgery, use of intermittent IV paracetamol reduces the median weight-adjusted cumulative morphine consumption in the first 48 h after surgery by 79% with equal pain relief showing equipoise for IV paracetamol as primary analgesic. Trial Registration Clinicaltrials.gov, Identifier: NCT05853263; EudraCT Number: 2015-001835-20.
Keywords: Analgesia; Child; Congenital cardiac surgery; Congenital heart defects; Intravenous paracetamol; Morphine; Randomized controlled trial.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Comment in
-
Beyond opioids: revisiting pain management in post cardiac surgery infants.Crit Care. 2024 Jun 7;28(1):193. doi: 10.1186/s13054-024-04983-3. Crit Care. 2024. PMID: 38849911 Free PMC article. No abstract available.
References
-
- Smith HAB, Besunder JB, Betters KA, Johnson PN, Srinivasan V, Stormorken A, et al. 2022 Society of critical care medicine clinical practice guidelines on prevention and management of pain, agitation, neuromuscular blockade, and delirium in critically ill pediatric patients with consideration of the ICU environment and early mobility. Pediatr Crit Care Med. 2022;23(2):e74–e110. doi: 10.1097/PCC.0000000000002873. - DOI - PubMed
-
- Valentine K, Cisco MJ, Lasa JJ, Achuff BJ, Kudchadkar SR, Staveski SL. A survey of current practices in sedation, analgesia, withdrawal, and delirium management in paediatric cardiac ICUs. Cardiol Young. 2023:1–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
- 836041016/ZONMW_/ZonMw/Netherlands
LinkOut - more resources
Full Text Sources
Medical
